Download
1 / 61
620 likes | 800 Views
Infra- glottic invasive airways. Dr. S.A.Rajkumar , Intensivist , Tirunelveli . Introduction. Airway access can be Supra- Glottic Infra- Glottic Routine ET intubation is by supra- glottic Alternative access to airway includes supra- glottic and infra- glottic access. Definition.

E N D
Infra-glotticinvasive airways Dr. S.A.Rajkumar, Intensivist, Tirunelveli.
Introduction • Airway access can be • Supra-Glottic • Infra-Glottic • Routine ET intubation is by supra-glottic • Alternative access to airway includes supra-glottic and infra-glottic access
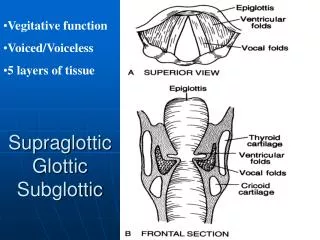
Definition • Supra-Glottic airway access Access to the airway by any means from the upper part of glottis into the trachea for ventilation or maintenance of airway. • Infra-Glottic airway access Access to the airway by means of opening the trachea below the glottis for ventilation or maintenance of airway. Non-invasive & Invasive Invasive
Infra-Glottic Airway Access • Broad classification: • CricothyrotomyTracheostomy • Access to them by: • Percutaneously Surgically
Infra-Glottic Airway Access • Done usually for: • Emergency ICU patients • situations • CNV / CNI • Conditions • when the airway access becomes an emergency procedure • For airway access or maintenance of airway
CNV / CNI • Could Not Ventilate / Could Not Intubatecondition [airway can not be maintained by either mask ventilation or intubation] warrents emergency methods of alternative airway access. • Required in • OT • Emergency ward • ICU • other departments as an emergency
History • 3000 years ago – India and Egypt • 1300 years ago – Spanish person Vesalius • Upto 1970 – Chavelier Jacksonadvised against Percutaneous procedures. • After 1970 invent of Ciagliadilatational techniques and Cooksdilational set, these were popularised. • Fiberopticbronchoscopy - safety
Techniques • Percutaneous jet ventilation (through needle) [and needle ventilation] • Retrograde intubation • Percutaneouscricothyrotomy • Percutaneoustracheostomy • Surgical cricothyrotomy • Surgical tracheostomy
Cricothyroid Membrane (CTM) • Between thyroid cartilage above and cricoid cartilage below. • 1 cm in height and 2 cm in width. • Central part – thick and triangular shape with apex below. (Conuselasticus) • Does not calcify with age. • Upper part of membrane – vascular anastamosis.
Tracheal Rings • Usual entry between 2nd and 3rdring or 3rd and 4th ring. • Tracheal rings are cartilagenous in front and membraneous behind. • Space between the rings is 1-2 mm. (but expandable) • Thyroid gland comes in front. • Innominate artery arches below.
Anaesthesia • IV sedation • Midazolam • Fentanyl / other narcotics • Propofol • Topical 1% Lidocaine – Intratracheal • Nerve blocks • Superior Laryngeal nerve • Glossopharyngeal nerve
Percutaneous Jet Ventilation • Transtracheal Jet ventilation (TTJV) • Used in • CNV / CNI situations • Surgeries of upper airways • Interim procedure till ET is placed • 12 – 16 G needle • High pressure O2 source [0.8 – 4 bar] • O2 concentration 30 – 100 % • I:E ratio = 1:1 • Ventilation frequency = 150 cycles per second • Venturi principle involves
Retrograde Intubation • Translaryngeal guided intubation • Popularised by Waters in 1963. Indications: • CNV / CNI condition • upper airway trauma • bleeding and secretions – unable to see glottis Relative Contraindications: • unfavourable anatomy (obesity, enlarged thyroid) • laryngotracheal diseases • coagulopathy • infection
Retrograde Intubation - Routine Technique Procedure • Through CTM epidural needle is pierced.
Retrograde IntubationRoutine Technique • Epidural catheter is inserted into oral cavity. • Catheter tip is taken out of mouth.
Retrograde IntubationRoutine Technique • ET tube railroaded and pulled into the trachea with the help of catheter.
Retrograde IntubationRoutine Technique • Then the epidural catheter is removed from the oral end.
Retrograde IntubationRoutine Technique • Now the ET tube is kept in situ.
Retrograde Intubation - Silk Pull-Through Technique • Here silk is threaded with the help of the epidural catheter.
Retrograde IntubationSilk Pull-Through Technique • Silk is tied at Murphy’s eye of ET tube
Retrograde IntubationSilk Pull-Through Technique • ET tube is placed into the trachea with the help of pulling of silk
Retrograde IntubationSilk Pull-Through Technique • Advantage: Reintubation is easy
Retrograde Intubation Complications: • esophageal perforation • hemoptysis • hematoma • edema • laryngospasm • infection, tracheitis • tracheal fistula • vocal cord damage • subcutaneous emphysema
PercutaneousCricothyrotomy • Definition: Cricothyrotomy can be defined as a technique for providing an opening in the space between the anterior inferior border of the thyroid cartilage and the anterior superior border of the cricoid cartilage for the purpose of gaining access to the airway. • Other names: sconiotomy, scricothyroidotomy, scricothyrostomy, sintercricothyrotomy, sminitracheostomy and spercutaneous dilatational tracheostomy.
PercutaneousCricothyrotomy Indications: • failed intubation • head and neck trauma • acute respiratory obstruction • alternative to tracheostomy It is done as an emergency procedure • during transport of patients • in the prehospital scenario • in the emergency department • in ICU • in OT
PercutaneousCricothyrotomy Relative Contraindications: • intubated patients (> 3 days) - subglotticstenosis • infants and children (< 10 years) - narrow airway • preexisting laryngeal disease • bleeding disorders
PercutaneousCricothyrotomy Techniques • Melkerpercutaneousdilationalcricothyrotomy device • Pertrachpercutaneousdilationalcricothyrotomy device (guidewire and dilator are in a single unit) • Nutrakepercutaneousdilationalcricothyrotomy device • Portex and MelkerMilitary (without guidewire) device [Used in emergencies In expert hands – 90 seconds (Ref: Benumof)]
PercutaneousCricothyrotomy- Technique • entry through the CTM.
PercutaneousCricothyrotomy- Technique • usually horizontal incision of skin.
PercutaneousCricothyrotomy- Technique • entry by 14 Fr. introducer and 17 G needle. • the position is confirmed by air aspiration.
PercutaneousCricothyrotomy- Technique • then guidewire is inserted into trachea.
PercutaneousCricothyrotomy- Technique • serial dilator or horn like single dilator or tracheostomy tube loaded dilator.
PercutaneousCricothyrotomy- Technique • now the tracheostomy tube is kept in situ.
PercutaneousCricothyrotomy Complications • Early: • asphyxia • hemorrhage • improper or unsuccessful tube placement • subcutaneous emphysema • pneumothorax • esophageal / mediastinal perforation • vocal cord injury • Late: • tracheal / subglotticstenosis • TE fistula • infection • tracheomalacia
PercutaneousTracheostomy • Definition: Tracheostomy can be defined as a technique for providing an opening in the space between any two tracheal rings (usually between 2nd and 3rd or 3rd and 4th rings) for the purpose of gaining access to the airway. • Except the entry point it is same like cricothyrotomy. Yet because of entry point there are some basic differences between two.
PercutaneousTracheostomy Indications: • usually done in ICU patients for • continuation of airway maintenance • weaning from ventilator • obstruction in airway • tracheal toileting • in children • in emergency situations • also in elective conditions (as Cricothyrotomy is not given preference in children)
PercutaneousTracheostomy Relative Contraindications: • midline neck mass (including thyroid) • high innominate artery • inability to palpate cricoid and trachea • unprotected airway • with PEEP > 20 cmH2O • coagulopathy [Now it is recommended to use fiberoptic bronchoscope to add safety to this procedure.]
PercutaneousTracheostomy- Technique • after adequate analgesia incision of skin over trachea is made at the access site.
PercutaneousTracheostomy- Technique • needle position is confirmed by aspiration of air as well as fiberoptic viewing of trachea.
PercutaneousTracheostomy- Technique • through 14 G needle a guidewire is inserted.