Download
1 / 50
560 likes | 1.26k Views
Chapter 28 The Urinary System. Urinary System Functions. Filtering of blood: involves three processes- filtration, reabsorption, secretion. Regulation of Blood volume Concentration of blood solutes: Na + , Cl - , K + , Ca 2+ , HPO 4 -2 pH of extracellular fluid: secrete H +

E N D
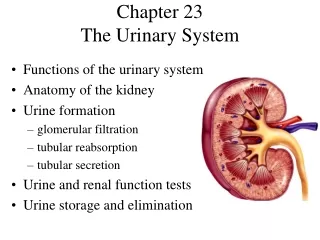
Urinary System Functions • Filtering of blood: involves three processes- filtration, reabsorption, secretion. • Regulation of • Blood volume • Concentration of blood solutes: Na+, Cl-, K+, Ca2+, HPO4-2 • pH of extracellular fluid: secrete H+ • Synthesis of vitamin D
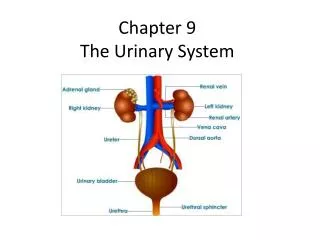
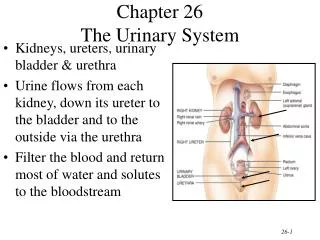
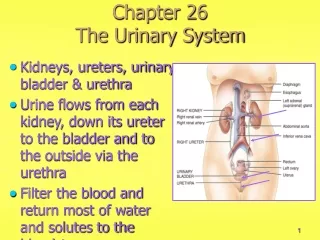
Location Lie behind peritoneum (retroperitoneal) on posterior abdominal wall on either side of vertebral column Lumbar vertebrae and rib cage partially protect Run from T12 –L3 Right kidney slightly lower than left External Anatomy Renal capsule: fibrous connective tissue. Surrounds each kidney Renal fat pad Engulfs renal capsule and acts as cushioning Renal fascia: thin layer loose connective tissue Anchors kidneys and surrounding adipose to abdominal wall Hilum Renal artery and nerves enter and renal vein and ureter exit kidneys Opens into renal sinus (cavity filled with fat and loose connective tissue) Location and External Anatomy of Kidneys
Internal Anatomy of Kidneys • Cortex: outer area • Renal columns: part of cortical tissue that extends into medulla • Medulla: inner area; surrounds renal sinus • Renal pyramids: cone-shaped. Base is boundary between cortex and medulla. Apex of pyramid is renal papilla, points toward sinus, base faces outward • Calyces • Minor: papillae extend into funnel of minor calyx • Major: converge to form pelvis • Pelvis: enlarged chamber formed by major calyces • Ureter: exits at the hilum; connects to urinary bladder
Anatomy and Histology of Ureters and Bladder • Ureters: bring urine from kidney to urinary bladder • Lined by transitional epithelium • Opens into the trigone • Composed of 3 tissue layers: inner mucous layer, muscular layer, fibrous outer layer • Trigone: interior of urinary bladder. Triangular area between the entry of the two ureters and the exit of the urethra. Area expands less than rest of bladder during filling. Clinically important site for bladder infections.
Anatomy of the Bladder and Urethra • Bladder • Muscular, collapsible bag between the pubis and the rectum • Women – anterior to the vagina and uterus • Men – sits on to of the prostate gland • Walls are formed by the detrussor muscle and transitional epithelium • Acts as a reservoir to urine and expels urine from the body • Urethra • Male: extends from the inferior part of the urinary bladder through the penis, moves through the prostate where it joins with 2 ejaculatory ducts • Female: shorter; opens into vestibule anterior to vaginal opening
Mechanism for Urination • Micturition • Increasing pressure causes involuntary contractions within the detrussor muscle triggered by PS reflexes • The internal urethral sphincter relaxes and micturition can occur if the external urethral sphinters relax • Voluntary control of micturition is only possible if the CNS projection tracts are developed • Not mature yet in infancy • Incontinence – involuntary micturition
Microscopic Structure • Nephrons • the microscopic functional units of the kidney • each nephron is made of two regions: • renal corpuscle • Glomerulus • Bowmans Capsule • renal tubule which connects to a shared collecting duct • Proximal convoluted tubule • Henle loop • Distal convoluted tubule • Collecting duct
Renal Corpuscle • Bowman’s capsule: • Cup shaped part of the nephron in which filtrate enters to form urine • outer parietal (simple squamous epithelium) and visceral (cells called podocytes) layers • Podocytes form narrow filtration slits lined with fine CT slit diaphragm • Glomerulus: network of capillaries. Blood enters through afferent arteriole, exits through efferent arteriole • Thin walls composed of fenestrations • Mesangial cells provide support/phagocytic role
Renal corpuscle • Basement membrane lies between the glomerulus and Bowman capsule • Glomerular capsular membrane: formed by glomerular endothelium, basement membrane, and the visceral layer of Bowman capsule; function is filtration
Renal Tubule and Collecting Ducts • Proximal tubule: simple cuboidal epithelium with many microvilli; cortex • Loops of Henle - medulla • Descending limb: first part similar to proximal tubule. Latter part becomes thinner • Ascending limb: first part is thin, distal part thicker • Length is important in determining the concentration of urine • Distal tubule: shorter than proximal tubule, conducts filtrate out of the nephron into the collecting duct, cortex • Collecting ducts: form where many distal tubules come together. Larger in diameter, lead to papillary ducts, release urine into calices, medulla
Circulation in the Glomerulus • Afferent arteriole: supplies blood to glomerulus • Efferent arteriole: drains glomerulus • Both vessels have a layer of smooth muscle • Juxtaglomerular apparatus: • Where the afferent arteriole passes by the distal tubule • sight of renin production when BP in the afferent arteriole drops • Juxtaglomerular cells- ring of smooth muscle cells in the afferent arteriole that produce renin • Macula densa- Specialized tubule cells of the distal tubule which sense changes in solute concentration The distal tubule lies between the afferent and efferent arterioles.
Circulation Through the Kidney Arterial supply: • Renal arteries branch from abdominal aorta • Segmental arteries branch from renal • Interlobar arteries ascend within renal columns toward cortex • Arcuate arteries branch and arch over the base of the pyramids • Interlobular (Cortical) arteries project into cortex and give rise to afferent arterioles
Circulation Through the Kidney • The part of the circulation involved with urine formation • Afferent arterioles supply blood to glomerulus • Glomerulus • Efferent arterioles exit the renal corpuscle • Peritubular capillaries form a plexus around the proximal and distal tubules • Vasa recta: specialized parts of peritubular capillaries that course into medulla along with loops of Henle, then back toward cortex, blood flows very slow through these capillaries
Circulation Through the Kidney • Venous drainage • Peritubular capillaries drain into interlobular (Cortical) veins and lead to • Arcuates • Interlobar veins • Renal veins
Types of Nephrons • Cortical nephrons- 85% of all nephrons • Renal corpuscle nearer to the periphery of the cortex. Loops of Henle do not extend deep into the medulla. • Juxtamedullary nephrons. Renal corpuscle near the cortical medullary border. Loops of Henle extend deep into the medulla.
Physiology • Overview of kidney function • Chief functions of the kidney are to process blood and form urine • Basic functional unit of the kidney is the nephron; forms urine by three processes (Figure 28-18) • Filtration: movement of water and protein-free solutes from plasma in the glomerulus into the capsular space of Bowman capsule • Tubular reabsorption: movement of molecules out of the tubule and into peritubular blood • Tubular secretion: movement of molecules out of peritubular blood and into the tubule for excretion
Filtration • Occurs in the renal corpuscles • Blood flows through the capillaries in the glomerulus, and water and solutes are forced out into Bowman’s capsule due to hydrostatic pressure • Filtrate: water, small molecules, ions that can pass through membrane • Mechanisms influencing filtration • Occurs due to pressure difference across filtration membrane • Systemic blood pressure and resistance to flow increase glomerular hydrostatic pressure • Osmotic pressure of glomerular blood plasma and hydrostatic pressure of the capsular filtrate resist filtration • Effective filtration pressure =glomerular hydrostatic pressure – (glomerular osmotic pressure + capsular hydrostatic pressure)
Filtration • Glomerular filtration rate (GFR): rate of movement of fluid out of the glomerulus and into the capsular space • Depends on the EFP and systemic blood pressure • Stress can cause constriction of afferent arteriole, decreasing glomerular hydrostatic pressure • Decrease in systemic blood pressure will decrease the GFR
Filtration • During diseases like glomerular nephritis, proteins enter the filtrate and filtrate exerts an osmotic pressure, increasing volume of filtrate (Box 28-3) • High glomerular capillary pressure results from • Low resistance to blood flow in afferent arterioles • Low resistance to blood flow in glomerular capillaries • High resistance to blood flow in efferent arterioles: small diameter vessels • Changes in afferent and efferent arteriole diameter alter filtration pressure • Dilation of afferent arterioles/constriction efferent arterioles increases glomerular capillary pressure, increasing filtration pressure and thus glomerular filtration
Tubular Reabsorption: Overview • Tubular reabsorption: occurs as filtrate flows through the lumens of proximal tubule, loop of Henle, distal tubule, and collecting ducts • Most reabsorption occur in the proximal tubule • Results because of • Diffusion • Facilitated diffusion • Active transport • Cotransport • Osmosis
Reabsorption in the PCT • Ion reabsorption and Osmosis • Na+ is actively transported out of the tubular lumen and into the blood • The IF becomes temporarily “+”, creating an electrical gradient, attracting “–” ions into the IF • The blood becomes hypertonic with the influx of ions drawing water into the capillaries via osmosis
Reabsorption in the PCT • Nutrient reabsorption • Glucose and aa move from the tubules back into the blood via sodium cotransport • Normally very little glucose is lost in the urine (exception = DM) • Max capacity for moving glucose depends on the carriers available • Urea • N – containing waste from protein catabolism • Half the urea content in the tubule passively diffuses into the blood down a concentration gradient
Summary of Reabsorption in Proximal Tubule • Sodium: actively transported out of tubule fluid and into blood • Glucose and amino acids: passively transported out of tubule fluid by sodium cotransport mechanisms; transport maximum is the maximal capacity of reabsorption and depends on carrier availability • Chloride, phosphate, and bicarbonate ions passively move into blood because of an imbalance in electrical charge • Water: movement of sodium and chloride into blood causes an osmotic imbalance, moving water passively into blood • Urea: approximately half of urea passively moves out of the tubule, with the remaining urea moving on to the Henle loop
Reabsorption in the Henle Loop • Countercurrent mechanism occurs between the Henle loop in juxtaglomerular nephrons and its vasa recta • Countercurrent because the contents of the ascending and descending limb are moving in different directions; arterial blood flows down and venous blood flows up vasa recta • Keeps solute concentration in the medulla high • Ascending and descending limb differences • Thin descending limb allows for water and urea to diffuse out of the tubule • Thick Ascending limb limits diffusion and actively transports molecules into the IF
Reabsorption in the Henle Loop • Thick ascending limb • Pumps Na+ and Cl- out of the tubule in the same manner as the PCT • The ions can’t diffuse back and are trapped in the IF • Normally, water would move out to follow the ions, but the ascending limb is impermeable to water • Solute concentration decreases in the tubule creating low osmotic pressure in the tubule and high osmotic pressure outside of the tubule • Countercurrent multiplier mechanism: • Henle loop concentrates sodium and chloride in the interstitial fluid of renal medulla
Reabsorption in the Henle Loop • Thin descending loop • The IF has a high solute concentration created by the Na+ and Cl- pumped out of the ascending loop, drawing water out of the descending loop • Solute concentration within the limb increases moving down • Urea diffuses into the descending limb, further increasing the solute concentration • Fluid enters the descending loop at 300mOsm and leaves the ascending loop at 100mOsm
Reabsorption in the Henle Loop • Countercurrent exchange mechanism in vasae rectae maintains high solute concentration in medullary interstitial fluid • Walls are permeable to water and to solutes: as blood flows toward medulla, water moves out, solutes diffuse in. As blood flows back toward cortex, water moves into vasa recta, some solutes diffuse out • Diffusion is such that slightly more water and slightly more solute are carried from the medulla by the vasa recta than enter it
Loops of Henle and vasa recta function together to maintain a high concentration of solutes in the interstitial fluids of the medulla and to carry away the water and solutes that enter the medulla from the loops of Henle and collecting ducts • Water moves out of descending limb and enters vasa recta • Solutes transported out of thick segment of ascending enter the vasa recta • Excess water and solutes carried away from medulla without reducing high concentration of solutes • Concentration of filtrate reduced to 100 mOsm/kg by the time it reaches distal tubule
Reabsorption in Distal Tubule and Collecting Duct • DCT reabsorbs some Na+ by active transport, but water cannot follow since the walls are impermeable to water; solute concentration continues to decrease • The collecting duct is also impermeable to water • Without any other outside influences, this would result in very hypotonic urine causing the body to dehydrate • A regulatory mechanism secretes ADH to target the DCT and CD increasing their permeability to water • The more ADH present, the more water that is reabsorbed into the blood and the more concentrated the urine • As more water moves out, the CD fluid becomes more concentrated, causing urea to move into the IF • Most of the urea diffuses into the descending LOH helping to maintain the high solute concentration in the medulla necessary to concentrate urine and avoid dehydration
Creating/Maintaining High Solute Concentration in Medulla • Active transport of Na+ and cotransport of ions such as K+ and Cl- and other ions out of the thick portion of ascending limb into interstitial fluid • Impermeability of thin and thick parts of ascending limb of loop of Henle to water • Vasa recta remove excess water and solutes that enter the medulla without destroying the high concentration of solutes in interstitial fluid of medulla • Active transport of ions from collecting ducts into interstitial fluid of medulla • Passive diffusion of urea from collecting ducts into interstitial fluid of medulla, impermeability of the ascending limb and permeability of the descending limb of the loops of Henle to urea
Tubular Secretion • Movement of substances out of the blood and into the tubular fluid • Moves metabolic by-products, drugs, molecules not normally produced by the body into tubule of nephron • K+, ammonium ions and H+ are secreted and removed in the tubule fluid via DCT and CD • Aldosterone targets the DCT and CD, increasing K+ secretion and Na+ absorption • H+ are secreted as blood pH decreases
Regulation of Urine Volume • Regulation of urine volume (Figure 28-27) • ADH influences water reabsorption; as water is reabsorbed, the total volume of urine is reduced by the amount of water removed by the tubules; ADH reduces water loss • Aldosterone, secreted by the adrenal cortex, increases distal tubule absorption of sodium, thereby raising the sodium concentration of blood and thus promoting reabsorption of water • Atrial natriuretic hormone, secreted by atrial muscle fibers, promotes loss of sodium by urine; opposes aldosterone, thus causing the kidneys to reabsorb less water and thereby produce more urine
Regulation of Urine Volume • Not normally altered by changes in the GFR • Tubuloglomerular feedback mechanism • maintains a constant GFR by regulating resistance in afferent arterioles; protects GFR function from rapid blood pressure variations • Dependent on macula densa cells and the juxtaglomerular apparatus which either speed up or slow down the GFR depending on the chemical concentration of the filtrate • may influence renin-angiotensin mechanism • Myogenic mechanism: rapid and effective regulation of GFR by changes in afferent arteriole smooth muscle contraction and relaxation • Urine volume: also related to the total amount of solutes other than sodium excreted in urine; in general, the more solutes, the more urine (DM)
Urine Composition • Urine composition: approximately 95% water with several substances dissolved in it; most important include: • Nitrogenous wastes: result of protein metabolism; include urea, uric acid, ammonia, and creatinine • Electrolytes: mainly the following ions: sodium, potassium, ammonium, chloride, bicarbonate, phosphate, and sulfate; amounts and kinds of minerals vary with diet and other factors • Toxins: during disease, bacterial poisons leave the body in urine • Pigments, especially urochromes • Hormones: high hormone levels may spill into the filtrate • Abnormal constituents (e.g., blood, glucose, albumin, casts, calculi)
Effects of Aging • Gradual decrease in size of kidneys, but only one-third of one kidney necessary for homeostasis • Amount of blood flowing through gradually decreases • Number of glomeruli decrease and ability to secrete and reabsorb decreases • Ability to concentrate urine declines and kidney becomes less responsive to ADH and aldosterone • Reduced ability to participate in vitamin D synthesis contributing to Ca2+ deficiency, osteoporosis, and bone fractures
Also… • Mechanisms of Disease • pp.969-973