Download

1 / 20
440 likes | 937 Views
The Healthcare System of the Netherlands. Lecture 6 Tracey Lynn Koehlmoos, PhD, MHA HSCI 609 Comparative International Health Systems. The Kingdom of the Netherlands. Population: 16.5 million (2006 est.) Capital: Amsterdam, but The Hague is the seat of government

E N D
The Healthcare System of the Netherlands Lecture 6 Tracey Lynn Koehlmoos, PhD, MHA HSCI 609 Comparative International Health Systems
The Kingdom of the Netherlands • Population: 16.5 million (2006 est.) • Capital: Amsterdam, but The Hague is the seat of government • Government: Constitutional Monarchy • Nationality: Dutch
Background Information • 12 provinces • Prosperous, stable, open economy heavily dependent on foreign trade. Low unemployment • Located at mouths of three major European rivers: Rhine, Maas, and Schelde • Founding member of NATO and the EU (now and participated in the introduction of the Euro in 1999
Updated Health Information • Life Expectancy: 76.4 m/ 81.7 f (2006) • Population over 65: 14.2 % (2006) • Infant Mortality: 4.96 per 1000 (2006) • Healthcare consumed 9.8% GDP (2003) • $ 2,976 (US) per capita health exp. (2003) • Major change took place in 2006, we must wait three or four years for the results
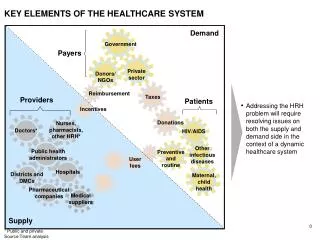
General Concepts • Long term, early adaptors of nationwide health education, healthy living and health promotion policies and ideals • Health (hence, healthcare) is universally regarded as a primary necessity • The Dutch healthcare system is a complex mix of public and private funding
Catalyst for Change • In former iterations the “Supply Driven” Dutch system was considered less than satisfactory by its users despite having relatively low cost and producing some of the BEST health outcomes measures in the world
Organization • Ministry of Public Health, Welfare and Sport (VWS) • Central planning authority • Responsible for implementing policy • Four basic “values” or characteristics • Strong supply side controls (wait lists) • Private character of supply • Mix of public and private financing • “Poldermodel”—political tradition of negotiation and consensus building
Big Changes to the System • Health Insurance Act went into effect 1 Jan 2006: • All Dutch citizens and all people working in the Netherlands MUST contract and carry health insurance • Only one period each year to switch enrollment • Established a Health Insurance Board to oversee the day-to-day running of the newly established “Health Insurance Fund”
3 Compartments of the new program • Health Insurance Fund • Self-selected/contractual health insurance • Mandatory w/ variable cost and levels of coverage • Some use cost containment co-pays, higher premiums • Exceptional Medical Expenses Fund • Long term, mental illness, chronic disability • Mandatory • Supplemental Insurance--optional
Financing the Health Insurance Funds • 50% Employer contributions • Employee or insurance enrollee paid “nominal premiums” • The IRS (Inland Revenue Service) assists the low income and the young (<18 years) • Previously, some 63% of Dutch citizens qualified for some form of public assistance
Health Insurers? NO! • In order to get the social message to health insurance companies, they have been renamed as “care insurers” • The insured have a “vote” in the corporation and changes • Insurers can offer a US style “managed care” plan or a traditional fee-for-service plan • Insurers cannot turn away applicants—no cherry picking, no exclusions
2005 Expenditures • In 2005, under the old system the Dutch spent approximately 45,895,000 Euros on healthcare • 37.7% “curative care” • 24.9% “elderly care” • 9.7% medications • 2.7% administration • .5% was on “prevention and promotion”
Health Services Workforce • More than 1 million people work in the healthcare sector • 3.1 physicians per 1000 per population • 2:1 GP to Specialists • Physician supply is controlled by a lottery system for medical school appointments • Most physicians are in private practice • Primary care physicians serve as gate keepers to hospital-based specialists • Physicians are paid via fee-for-service, capitation, or a mix
Health Services Workforce • 12.8 Nurses per 1000 population • Considered a full-fledged profession • Low salaries, dissatisfaction with low status • Hospital specialists and community nurses • >18% male nurses • Many work like PA or in high-tech • No mid-level practitioners
Health Services Workforce • Health Administrators • Long standing tradition • Several universities offer undergraduate and graduate degrees • With the collective approach to deciding any issue, it is important to have administrators who have a wide-expanse of knowledge: policy, problem solving, social science, law & economics
Hospitals • Like US, Canada—switched from lengthy inpatient stays to more ambulatory and outpatient care • <400 hospitals in the Netherlands • Most are private, not-for-profit (religious affiliation) • Traditionally paid through annual global budgeting, but the new system will allow for market competition between hospitals
Long-term Care • Combination of social and health services • More emphasis on home based care • Care providers work with manpower services, welfare agencies and industry • Dutch municipalities provide transportation and special equipment (like wheelchairs) to elderly and disabled residents
Could we go to Amsterdam and not talk about drugs? • Drugs!?! • Ministry of Health, Welfare and Sport controlled policy to prevent drug use and trafficking • Distinction between cannabis and hard drugs (lowest drug death rate in Europe) • Prescription drugs? • Mostly covered under “care insurer” formularies • Some co-pays, option to pay more for different drugs
Compared to US • Long-term Care: Dutch have the best system in the world for taking care of the elderly also well-equipped for mental illness and substance abuse • Universal, private insurance of choice • All access system • Higher Physician to Population ration than US • General practitioners make ½ of US GP’s
Summary • The Netherlands entered into a completely new healthcare system in 2006 • Everyone must carry two types of private insurance (long term/catastrophic & curative) • Emphasis on managed market competition in the health sector • It will be years (2009?) before we can accurately measure the results of this change