Download
1 / 35
350 likes | 447 Views
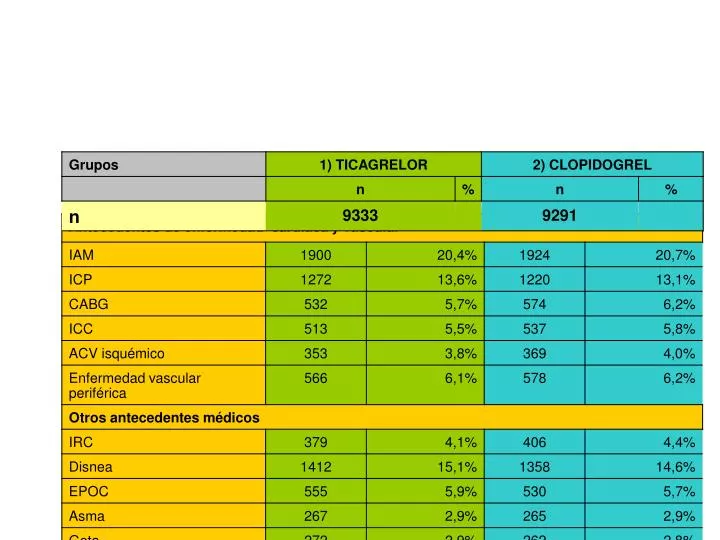
RESULTADOS: CARACTERÍSTICAS BASALES. RESULTADOS: CARACTERÍSTICAS BASALES. RESULTADOS: CARACTERÍSTICAS BASALES. RESULTADOS: CARACTERÍSTICAS BASALES. RESULTADOS: CARACTERÍSTICAS BASALES. RESULTADOS: CARACTERÍSTICAS BASALES. RESULTADOS: CARACTERÍSTICAS BASALES.

E N D
RESULTADOS: END POINT PRIMARIO Beneficio atenuado en: Menor peso (P=0,04). No hipolipemiantes (p=0,04). Randomizados en Norteamérica.
RESULTADOS: END POINTS SECUNDARIO PRINCIPAL (PACIENTES SOMETIDOS A ESTRATEGIA INVASIVA)
DISCUSIÓN: • Ticagrelor vs clopidogrel: ↓ † de causa vascular, IAM o ACV. ↓ † de causa vascular, IAM individualmente, no ACV. Beneficio independiente de CG. ↓ † de cualquier causa ↓ riesgo de fenomenos tromboticos sin ↑ riesgo de sangrado mayor.
DISCUSIÓN: • Ticagrelor vs clopidogrel: ↑ de sangrado espontáneo. ↑ HIC fatal, pero ↓ sangrado fatal no intracraneal, ↓ † cv u otra causa ↓ total †. Disnea muy frecuente (13,8%) abandono 0,9%. Primera semana + pausas ventriculares.
DISCUSIÓN: • Ticagrelor: Efecto reversible se podría usar en pacientes que van a ser sometidos a CABG o en pacientes cuya anatomía coronaria se desconoce. Posología cada 12 horas. Evitar en pacientes con historia de ACV/AIT, riesgo excesivo de sangrado. Cuidado en pacientes OCFA, hiperuricemia, IR, bradiarritmias sin MP, H de síncope, necesidad de tratamiento con antiagregantes > 1 año. ¿Efecto reversible desventaja? ttos crónicos. No diseño para demostrar diferencias en la mortalidad: ¿real? ¿magnitud?
INTRODUCCIÓN: PRASUGREL. TRIAL TO ASSESS IMPROVEMENT IN THERAPEUTIC OUTCOMES BY OPTIMIZING PLATELET INHIBITION WITH PRASUGREL
TRIAL ORGANIZATION Trial Leadership: TIMI Study Group Eugene Braunwald,Chairman, Elliott M. Antman,PI, Stephen D. Wiviott, Gilles Montalescot, Carolyn H. McCabe, Sabina A. Murphy, Susan McHale Sponsors: Daiichi Sankyo and Eli Lilly J. Anthony Ware, Jeffrey Riesmeyer, William Macias, James Croaning, Govinda Weerakkody, Francis Plat, Tomas Bocanegra Data Center and Site Management: Quintiles Inc Data Safety Monitoring Board David Williams (Chair) , Christophe Bode, Spencer King, Ulrich Sigwart, David DeMets
ESTUDIO: ACS (STEMI or UA/NSTEMI) & Planned PCI N= 13,600 ASA Double-blind CLOPIDOGREL 300 mg LD/ 75 mg MD PRASUGREL 60 mg LD/ 10 mg MD Median duration of therapy - 12 months 1o endpoint: CV death, MI, Stroke 2o endpoints: CV death, MI, Stroke, Rehosp-Rec Isch CV death, MI, UTVR Stent Thrombosis (ARC definite/prob.) Safety endpoints: TIMI major bleeds, Life-threatening bleedsKey Substudies: Pharmacokinetic, Genomic
Enrollment: Nov 2004 - Jan 2007N = 13,608 (ITT) 30 Countries 707 Sites
Enrollment Criteria • Inclusion CriteriaPlanned PCI for : Mod-High Risk UA/NSTEMI (TRS > 3) STEMI: < 14 days (ischemia or Rx strategy) STEMI: Primary PCI • Major Exclusion Criteria: • Severe comorbidity • Increased bleeding risk • Prior hemorrhagic stroke or any stroke < 3 mos • Any thienopyridine within 5 days • No exclusion for advanced age or renal function KnownAnatomy
Baseline Characteristics *P<0.05
PrimaryEndpointCVDeath,MI,Stroke 15 Clopidogrel 12.1(781) 9.9 (643) 10 Primary Endpoint (%) Prasugrel HR 0.81(0.73-0.90)P=0.0004 HR 0.80P=0.0003 HR 0.77P=0.0001 5 NNT= 46 LTFU = 14 (0.1%) ITT= 13,608 0 90 0 180 30 270 360 450 Days
TRITON TIMI 38 Bleeding events:Safety cohort n = 13,457 Clopidogrel Prasugrel ICH in patients with prior stroke/TIA (n = 518) 4 Clopidogrel 0 (0%) Prasugrel 6 (2.3%)(P = 0.02) 2.4 Events (%) 1.8 2 1.4 1.1 0.9 0.9 0.4 0.3 0.3 0.1 0 TIMImajor Life- Non-fatal Fatal ICH bleeds Threatening ARD 0.6%HR 1.32P = 0.03NNH = 167 ARD 0.5%HR 1.52P = 0.01 ARD 0.2%P = 0.23 ARD 0.3%P = 0.002 ARD 0%P = 0.74
TRITON TIMI 38 Total Events Prevented: First and Recurrent Total EventsP<0.0001 896 -195 701 AdditionalEvents # Events 1st EventP=0.0004 -138 Prasugrel Clopidogrel ITT N= 13,608
Net Clinical BenefitDeath, MI, Stroke, Major Bleed (non CABG) Events per 1000 pts + Major Bleed(non CABG) MI 15 Clopidogrel 13.9 ITT= 13,608 12.2 HR 0.87P=0.004 Prasugrel 10 Endpoint(%) All CauseMortality 5 Clop 3.2%Pras 3.0 %P=0.64 0 0 30 60 90 180 270 360 450 Days
Diabetic Subgroup N=3146 18 Clopidogrel 17.0 16 CV Death / MI / Stroke 14 12.2 12 HR 0.70P<0.001 Endpoint(%) Prasugrel 10 NNT = 21 8 6 TIMI Major NonCABG Bleeds Clopidogrel 4 2.6 2.5 2 Prasugrel 0 0 30 60 90 180 270 360 450 Days
Comparison with Higher Dose Clopidogrel IPA (%; 20 M ADP) IPA (%; 20 M ADP) P<0.0001 N=201 P<0.0001 for each Prasugrel 60 mg Clopidogrel 600 mg Clopidogrel 150 mg Prasugrel 10 mg Hours 14 Days Wiviott et al Circ 2007 (In Press)
Efficacy 1. A significant reduction in: CV Death/MI/Stroke 19% Stent Thrombosis 52% uTVR 34% MI 24% 2. An early and sustained benefit 3. Across ACS spectrum Safety Significant increase in serious bleeding(32% increase)Avoid in pts with prior CVA/TIA ConclusionsHigher IPA to Support PCI Prasugrel 60 mg LD/10mg MD vs Clopidogrel 300 mg LD/ 75 mg MD Net clinical benefit significantly favored Prasugrel

