Download
1 / 23
240 likes | 594 Views
The biology of window period infections: implications for donor screening and inventory hold. Dr. Steven Kleinman FDA BPAC meeting September 21, 2001 . Sources of residual risk. Infectious, window period donations

E N D
The biology of window period infections: implications for donor screening and inventory hold Dr. Steven Kleinman FDA BPAC meeting September 21, 2001
Sources of residual risk • Infectious, window period donations • time between infectivity and detection with screening tests (may be different from time of exposure to an agent) • Viral variants (strains, subtypes) not detected by current tests • Infectious chronic antibody neg carriers • Errors (testing or product release)
Events in early viral infection WP1 WP 2 Serological Exposure Infectivity Detection Eclipse Viremia
Stages of Infectivity • Surrogate for infectivity is viremia detectable by NAT (PCR) • Can define four stages of viremia • Pre-ramp up • Ramp-up (exponential increase) • Plateau phase • Post-seroconversion phase
Pre-ramp-up Viremia • Low-level, intermittent “blips” detected prior to quantifiable ramp-up phase • Significance not yet understood • Inoculum vs focal replication that seeds dissemination vs abortive replication (transient w/o subsequent ramp-up/SC) • Is this viremia infectious?
Immunosilent carriers: chronic antibody negative carriers • Persistent viremia in absence of detectable seroconversion • Case reports for HIV, HCV, and HBV • Recipient infection via transfusion has been documented for HCV • Appears to be rare
Estimates of false negative test error rates in routine donor screening • 1 of 2,015 (0.05%) confirmed seropositive donors tested negative (due to technical testing error) on a subsequent donation (Busch et al. Trans. 2000) • 3 of 2,307 (0.13%) HCV seropositive donations to ARC were originally missed and identified by retesting due to positive NAT results (none have subsequently been reported)
Sources of window period data • Defined parenteral exposures (needlestick injury, transfusion) • Plasma seroconversion panels • Source of infection and date of exposure is unknown • Source is inferred to be IVD, sexual, or another (uncommon) mode
Estimates for WPs from Exposure to Seroconversion Following Discrete Parenteral Exposures
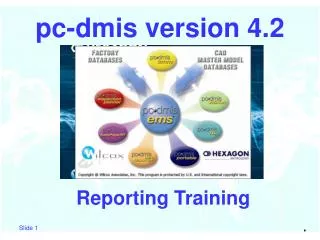
HIV needlestick exposure • 95% of cases seroconverted within 6 months of exposure • The delayed seroconverters were viremic for only a short time prior to seroconversion • Infectivity may be confined to this short time interval
0 10 20 30 40 50 60 70 80 90 100 HIV markers during early infection HCV RNA (plasma) DT = 21.5 hrs HIV Antibody HIV p24 Ag 11 16 22 Theoretical Infectivity Day 0HIV RNA Day 11 HIV p24 Ag Day 16 HIV Antibody Day 22 5 Days 6 Days
Time to Detection of Transfusion-Transmitted HCV Infection (n=28) Time toMean95% CI RNA 12.6 1.5-23.7 ALT 51.5 18.5-84.5 EIA3.0 70.7 32.8-128.6
HCV markers during early infection Plateau phase = 57 days DT= 17.7 hrs HCV RNA Anti-HCV 12 0 10 20 30 40 50 60 70 80 90 100 Infection Day 0 HCV RNA Day 12 HCV Antibody Day 70
Duration of Viremic WPs Prior to SC Detectable by MD and ID-NAT * * Assumes sensitivity of ID NAT = 50 gEq / mL, and MP NAT = 1000 gEq / mL ** Does not include detection of intermittent, low-level viremic episodes preceding ramp-up viremia
Testing Algorithm for HCV NAT-conversion Panels Alpha Therapeutic / NGI screening (Antibody & 512 Pool PCR) 63 HCV NAT-conversion Panels ( 774 Donations ) 5 Control Panels ( 54 Donations ) dHCV TMA Testing Intermittent Pre-Ramp-Up Viremia * in 25/41 (61%) panels >3 pre-r/u units Ramp-Up & Plateau Phase Quantitative Viral Load ( Roche Monitor ) Replicate dTMA ( x 3 ) & NGI UltraQual PCR Testing * Ramp-Up = consistent RNA detection with progressive increase in viral load.
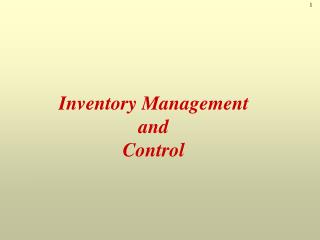
NGI 512 PCR x108 Neat PCR x107 HCV Monitor PCR (gEq/mL) % dTMA Positive (4 replicates) 100 x106 75 x105 50 x104 x103 25 x102 -60 -40 -20 0 10 20 Days Pre/Post 1st Quantitative RNA+ Donation Low-Level Intermittent HCV ViremiaPreceding Ramp-Up Phase Assay sensitivity (6 x 102) (BCP ID 10083)
HCV: Pre-ramp up viremia • Intermittent, low-level viremia preceded ramp-up phase viremia by up to 60 days • Statistical analysis of the duration of pre-ramp up viremia has not yet been performed • Significance for transmission by sexual route has not been determined
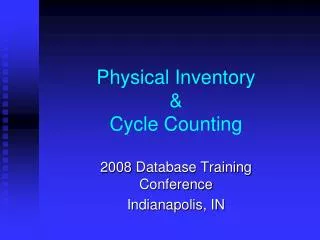
0 10 20 30 40 50 60 70 80 90 100 110 HBV markers during early infection HBV DNA (PCR) Anti-HBc HBsAg ALT Infection 59 120 Infection Day 0 HBV DNA Variable, up to 31 days prior to HBsAg by ID NAT( 9-11 days by MP NAT) HBsAg Day 59; disappears Day 120
Window Period Viremia Parameters Derived from NAT Analysis of Plasma Donor Panels * Based on follow-up of 30 plasma donors detected as MP-NAT-pos by Alpha and Bayer (95% CI 29-85 days)
HCV: immunosilent carriers • In over 2 years of NAT testing, ARC has identified 2 donors who were HCV RNA positive and did not develope HCV antibody in the subsequent 6 months • The denominator is over 12 million donations and an estimated 12,000 HCV antibody positive donations
ARC HCV NAT Reactive Donations Confirmed with Follow up Sample(s) N = 25 Seroreactive Seronegative Seroreactive, NAT Negative Seronegative, NAT Negative Number of Days
Risk and risk reduction calculations • Risk = Number of donors in infectious window period (Annual Incidence x WP as fraction of year) + Rate of silent carriers + Prevalence x Error rate • WP < 0.2 year for all viruses • Risk reduction = Annual Incidence x (reduction in WP) + Rate of silent carriers x (reduction factor) + Prevalence x (Reduction in error rate)
Interventions to decrease risk compared to single sample serologic screening Quarantine/ retestNAT Window Silent carrier no effect Testing error to 0 to 0 Quarantine risk reduction = Incidence x (95% to 100% reduction) + Silent carrier rate + Prevalence x (almost 100% reduction in error rate)