Download
1 / 25
250 likes | 357 Views
Male R eproductive Physiology . Dr. Amel Eassawi. Objectives. Describe the physiological functions of the major components of the male reproductive system. Explain how the secretions of FSH and LH are regulated in the male and describe the actions of these hormones.

E N D
Male Reproductive Physiology Dr. AmelEassawi
Objectives • Describe the physiological functions of the major components of the male reproductive system. • Explain how the secretions of FSH and LH are regulated in the male and describe the actions of these hormones. • Describe spermatogenesis and the role of Sertoli cells, Leydigcells. • Explain the hormonal control of spermatogenesis and describe the effects of androgens on the male accessory sex organs. • Discuss the mechanisms of erection and ejaculation. • Discuss the various factors that affect male fertility.
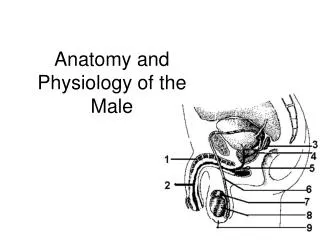
MALE REPRODUCTIVE System Primary Sex Organs: Testes Functional Compartments: • Seminiferous Tubules : Exocrine Function (spermatogenesis) • Interstitial Tissue: Endocrine Function: Leydigcells (interstitial cells). Androgen Secretion (mainly testerone)
Male Reproductive SYSTEM Testosterone • Steroid hormone. • Synthesized from the cholesterol precursor in the Leydig cells and also from the androstenedione secreted by the adrenal cortex. • Testosterone secretion rate is 4-9mg/dL in normal adults and very small amount is secreted in women.
Estrogen in Males Small amount produce by adrenal cortex A portion of the testosterone secreted by the testes is converted to estrogen outside the testes by the enzyme aromatase, which is widely distributed but most abundant in adipose tissue
Spermatogenesis 1. Complex process by which diploid primordial germ cells (spermatogonia) are converted into motile haploid spermatozoa (sperm). 2. It takes 64 days for development of mature sperm from spermatogonium (several hundred million sperm may reach maturity daily)
Spermatogenesis Spermatogenesis: Spermatids to Sperm
Spermatogenesis Spermatozoa: Consists of four parts • Head • Consists primarily of the nucleus (contains DNA) • Acrosome • containing hydrolytic enzymes that allow the sperm to penetrate and enter the egg • Midpiece • Area where mitochondria are concentrated • Tail • Provides mobility for spermatozoa
Functions of Sertoli cells • Form blood-testes barrier. • Provide nourishment and phagocytic function. • Secrete seminiferous tubule fluid which flushes released sperm from tubule into epididymis. • Secrete androgen-binding protein. • Site of action for testosterone & FSH to control spermatogenesis • Release inhibin, acts in negative-feedback fashion to regulate FSH secretion • Released mullerian inhibiting factor ( fetal development).
TESTICULAR CELL INTERACTIONS • Sertoli cell products estradiol, inhibin, activin and other proteins modulate leydig cell activity • Sertoli cell products modulate germ cell function • Leydig cell testosterone modulate peritubular & Sertoli cell function • Peritubular cell products influence Sertoli cell activity
Location and Functions of the Components of the Male Reproductive System
MALE SEXUAL PERFORMANCE Erection
MALE SEXUAL PERFORMANCE Mechanism of Penile Erection • Relaxation of trabecular smooth muscle leading to increased blood flow into cavernosalsinousoids • Engorged corpora cavernosa presses venules against tunica albuginea restricting venous outflow. Regulation of penile erection (smooth muscle tone) • Proerectile factors: parasympathetic input, intracellular Ca+2, PGE1, NO, smooth muscle sensitivity to Ca+2 • Antierection factors: sympathetic input intracellular Ca+2, NE, smooth muscle sensitivity to Ca+2
HUMAN SEXUAL RESPONSE CYCLE PHASES Phases include excitement, plateau, orgasm and resolution The resolution time for men is longer resulting in an increased refractory period to further stimulation
MALE SEXUAL PERFORMANCE Erectile dysfunction or Impotence: Failure to achieve or maintain an erection suitable for sexual intercourse. Affect 50% of men between 40 and 70 years old. May be due to: 1. Psychological factors. 2. Physical factors. A. Nerve damage B. Medication that interfere with autonomic function C. Problem with blood flow to the penis. Sildenafil (Vigra): prescribed to treat erectile dysfunction. It does not produce an erection but it amplifies and prolongs an erectile response triggered by usual means of stimulation.
GYNECOMASTIA • Defined as presence of any palpable breast tissue in men. • Due to increase in estrogen-androgen ratio. • Three classes physiological, pathological and idiopathic. • Three time period(Birth, Puberty, Old Age). • Pysiological • The breast enlargement of newborns, the transient gynecomastia of adolescence and breast development of aging men, which cannot be associated with a pathological condition are considered to be physiological. • Pathological • Hypogonadism (Klinefelters). • Chronic liver diseases (cirrhosis, hepatitis). • Thyrotoxicosis. • Neoplasia. • Drugs (estrogen, testosterone)
Abnormalities of testicular function 1. Cryptorchidism: descent of testes is incomplete, testes remain in the abdomen. Occurs in neonatal life. 1. Bilateral: Impaired Testosterone secretion and spermatogenesis. 2. Unilateral :Normal Testosterone and impaired spermatogenesis. 2. Male hypogonadism: Clinical picture depends on whether testicular deficiency develops before or after puberty. causes: • Testicular disease (Hypergonadotrophic Hypogonadism) • Disorder of hypothalamus or pituitary (Hypergonadotrophic Hypogonadism) 3. Androgen secreting tumors : Leydig cell tumors (a rare condition) leads to precocious pseudopuberty in prepubertal boys.
References • Human physiology, Lauralee Sherwood, seventh edition. • Text book physiology by Guyton &Hall,11th edition. • Text book of physiology by Linda .s Contanzo, third edition. • Physiology by Berne and Levy, sixth edition.