Download
1 / 35
350 likes | 638 Views
2. The urinary system consists of 2 kidneys, 2 ureters, 1 urinary bladder

E N D
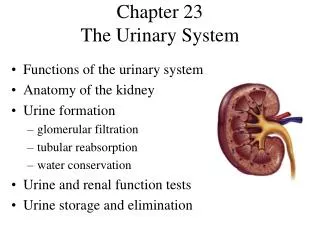
1. 1 CHAPTER 23
THE URINARY SYSTEM
KENNETH E. MULLER, PhD,PT
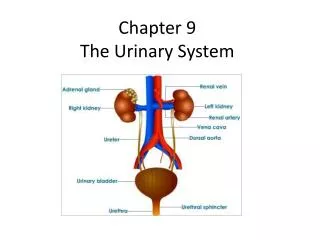
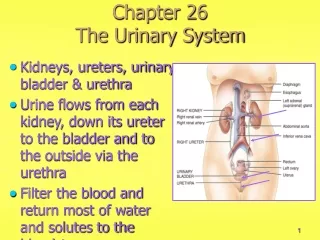
2. 2 The urinary system consists of 2 kidneys, 2 ureters, 1 urinary bladder & 1 urethra.
Urine is excreted through each kidney through the ureter and stored in the bladder until it is expelled through the urethra.
Nephrology- Study of the anatomy and physiology of the kidney.
Urology- Branch of medicine that deals with male and female urinary systems.
Functions of the kidneys-
Regulation of blood ionic composition
Regulation of Na+, Ca2+, Cl-, HPO4.
3. 3 Maintenance of blood osmolarity-
Regulates loss of water & loss of solutes in urine
Maintains constant blood osmolarity
Regulates blood volume-
Adjusts blood volume by conserving or eliminating water.
^ blood volume = ^ blood pressure
Regulates blood pressure-
Secrete the enzyme Renin which activates the REnin-Angiotensin pathway.
Adjusts resistance encountered by blood flowing through the kidneys which affects systemic vascular resistance.
An increase in Renin or an increase in vascular resistance>increased blood pressure.
4. 4 Regulates blood pH-
Excretes H+ and conserves HCO3-
Releases hormones
Calcitrol- the active form of vitamin D, which helps regulate calcium homeostasis.
Erythropoietin- Stimulates production of RBC�s
Regulates blood glucose-
Involved in breaking down the amino acid glutamine to be used in glucose synthesis.
Excretes wastes and foreign substances-
Forms urine from substances that have no useful function in the body.
5. 5 Kidney Anatomy-
Paired, reddish, kidney bean shaped. Located just superior to the waist between the peritoneum and the posterior abdominal wall.
The concave medial border faces the vertebral column.
Located between T12 and L3, right slightly lower than the left.
Renal Hilus- deep vertical fissure near the center of the concave border. Ureter, blood vessels, nerves and lymphatics leave through here.
6. 6 3 layers surround the kidney-
Renal Capsule- deepest layer, Smooth, transparent, fibrous membrane. Serves as a barrier against trauma and helps to maintain the shape of the kidney.
Adipose capsule- middle layer, mass of fatty tissue that surrounds the kidney.
Renal fascia- superficial layer, anchors the kidney to surrounding structures and to the abdominal wall.
Internal anatomy-
Renal Cortex- smooth textured, superficial, reddish area.
Renal medulla- deep, inner layer, reddish brown.
7. 7 Medulla consists of 8-18 cone-shaped renal pyramids
The wider base of each pyramid faces the renal cortex.
The narrower apex is called the renal papilla and points to the center of the kidney.
Renal columns- portions of the renal cortex that extend between the renal pyramids.
Parenchyma- functional portion of the kidney. Constitutes the cortex+ pyramids.
Nephron- functional unit of the kidney. Microscopic ~1 million of them.
8. 8 Papillary ducts- Urine formed in the nephron drains into the papillary ducts which extend in to the renal papilla of the pyramids.
Papillary ducts drain into the major and minor calyces. Each kidney has 8-18 minor and 2-3 major.
From the major calyces urine drains into a single cavity called the renal pelvis.
Renal sinus- Hilus expands into a cavity call the renal sinus.
Nerve & Blood supply-
Abundantly supplied with blood vessels. Kidneys receive 20-25% of the resting cardiac output. (The renal fraction) Blood flows through renal arteries ~1200 mL/min.
9. 9 Within the kidney each renal artery divides into several segmental arteries into interlobar arteries to arcuate arteries to interlobular arteries to afferent arterioles.
Each nephron receives one afferent arteriole which divides into the glomerulus.
Glomerulus- a tangled, ball shaped capillary network.
Efferent arteriole- Drains blood out of the glomerulus.
10. 10 Vasodialtion or constriction of the afferent or efferent arterioles cause changes in the renal blood flow and vascular resistance. Due to this the glomerulus is considered part of the cardiovascular and urinary systems.
Efferent arterioles divide to form a network of capillaries called the peritubular capillaries. Surrounds the tubular portion of the Nephron in the cortex.
Nerves of the kidney originate in the celiac ganglion. Part of the sympathetic division of the ANS.
11. 11 The Nephron- Functional unit of the kidney
Engage in 3 processes:
Filtering blood
Returns useful substances to the blood so they are not lost from the body.
Removes substances from the blood that are not needed by the body.
The Nephron maintains homeostasis of the blood and processes urine.
Parts of the Nephron:
Each Nephron consists of 2 portions-
Renal Corpulse- Where plasma is filtered. Has 2 Components-
Glomerulus
Boman�s capsule
12. 12 Renal tubule- where the filtered fluid passes. Has 3 main sections.
Proximal convoluted tubule
Loop of Henle- connects the proximal & distal convoluted tubule.
Distal convoluted tubule- Empties into collecting ducts.
Descending loop of Henle- 1st portion, dips into the renal medulla.
The loop makes a hairpin turn and returns as the ascending loop of Henle.
80-85% of Nephrons are cortical. Corpulses lie in the outer portion of the cortex and have short loops that barely enter the medulla.
13. 13 The other 15-20% are called juxtamedullary, lie deep in the cortex and have long loops which extend into the deepest part of the medulla.
Thin and thick ascending loops.
The number of Nephrons is constant from birth. Increase in kidney size is due to growth of the existing Nephron.
Surgical removal of one kidney causes hypertrophy of the remaining kidney which can eventually filter at 80% of the rate of 2 normal kidneys.
14. 14 Renal Physiology- 3 processes:
Glomerular filtration- 1st step in urine production. Water and solutes in plasma pass from blood across glomerular capillaries. Empty into the renal tubule.
Tubular reabsorption- Most filtered water and useful solutes are reabsorbed by tubule cells and returned to the blood through peritubular capillaries.
Tubular secretion- Tubule cells secrete wastes into the fluid. Tubular secretion removes unwanted substances from the blood.
15. 15 Solutes in the fluid that drain into the renal pelvis remain in the urine and are secreted.
Rate of urinary excretion = rate of glomerular filtration + rate of secretion- rate of reabsorption.
Glomerular filtration-
fluid that enters the capsular space is called glomerular filtrate.
Daily volume of GF ~180 L/day. More than 99% is returned to the bloodstream.
Glomerular endothelial cells have large fenestrations, quite leaky. Permits all solutes in blood plasma to exit glomerular capillaries but prevents filtration of blood cells and platelets.
16. 16 Filtration- uses pressure to force some of the fluids and solutes through a membrane.
Volume of fluid filtered is large due to 3 reasons:
Glomerular capillaries are long and present a large surface area for filtration.
The filtration membrane is thin & porous. 50 times leakier than capillaries in most other tissues.
Glomerular capillary blood pressure is high which produces more filtrate.
Dependent upon the filtration coefficient, ^ in males.
Glomerular filtration depends on 3 main pressures
Glomerular blood hydrostatic pressure ( BHP) - Promotes filtration. Forces H2O and solutes in plasma through filtration membrane. ~60mm Hg.
17. 17 NO MORE TONIGHT
LET�S GO HOME
18. 18 Capsular pressure (CP)- Opposes filtration. Pressure exerted against the filtration membrane by fluid already in the capsular space. ~18mmHg.
Colloid Osmotic Pressure (COP)- due to proteins such as albumin, globulins and fibrinoen in blood plasma. Opposes filtration. ~32mm Hg.
Net filtration pressure (NFP)-
NFP = BHP- CP - COP
NFP= 60 mmHg- 18 mmHg- 32 mmHg= 10 mmHg
This pressure causes a normal amount of plasma to filter the glomerulus into the capsular space.
19. 19 Glomerular filtration rate- ~120-125 mL/min
Homeostasis requires the GFR remain constant.
GFR is directly related to pressures that determine NFP. Severe blood loss reduces systemic BP and GBHP. Filtration ceases at 45mm Hg.
Regulation of GFR- works 2 main ways:
By adjusting blood flow into and out of the glomerulus.
By altering glomerular capillary surface area available for filtration.
GFR increases when blood flow into the glomerular capillaries increase.
20. 20 3 mechanisms control GFR:
Renal autoregulation
Neural regulation
Hormonal regulation
Renal autoregulation of GFR- 2 mechanisms
Myogenic mechanism- Stretching triggers contractionof smooth muscle cells in the wall of the afferent arteriole. ^BP = ^GFR
Tubuloglomerular feedback- When GFR is higher than normal, filtered fluid flows more rapidly through the renal tubules and stimulates the release of an unknown vasoconstrictor which cause the afferent arteriole to constrict. Less blood flows into the glomerular capillaries and GFR decreases.
21. 21 Neural regulation of GFR-
Kidneys are supplied by sympathetic ANS fibers that release norepinephrine. Causes vasoconstriction of alpha 1 receptors in the smooth muscle in the afferent arteriole.
At rest sympathetic stimulation is low. With significant sympathetic ie. Exercise, hemmorrage, blood flow into glomerular capillaries decreases which reduces urine output and conserves blood volume.
Sympathetic stimulation also stimulates the release of renin.
22. 22 Homonal regulation of GFR- Angiotensin II reduces GFR. Atrial natriuretic peptide (ANP) secreted by atria increase GFR.
Tubular reabsorption and secretion-
The volume of fluid entering the proximal convoluted tubule in 1/2 hour is greater than the total plasma volume.
Solutes reabsorbed include Na, K, Ca, Cl, HCO
Proximal convoluted tubule involved in the most reabsorption.
Fig 23.15 p 910
Fig 23.16 p 912
23. 23 Glucosuria- when blood glucose ^200 mg/mL some glucose will remain in the urine. Most common cause of diabetes mellitus.
The majority of solute and water reabsorption-
Most absorptive processes involve Na+
2 types of Na transporters are located in the PCT.
Na symporters effect Na reabsorption of Na together with a variety of other solutes. Filtered glucose, amino acids, lactic acid, water soluble vitamins, and other nutrients are completely reabsorbed in the 1st half of the PCT by Na transporters located in the membrane.
24. 24 Na/H+ antiporters- carry filtered Na down its concentration gradient into PCT cells in exchange for H+. Na is reabsorbed and and H+ is secreted. PCT cells continually produce H+ to keep the pump running.
Reabsorption of solutes in the PCT promotes reabsorption of water via osmosis. Concentration gradient must be equalized.
Ammonia (NH3) is a byproduct of deaminatioand is secreted into the tubular fluid at the PCT.
Reabsorption at the loop of Henle-
PCT reabsorbs-65% of the filtered water (80 mL/min) Fluid enters the LOH at ~40-45 mL/min. The LOH reabsorbs about 20-30% filtered Na, K+, Ca, 15% H2O
25. 25 Little or no water is reabsorbed in the ascending loop, all in the descending loop.
Distal Convoluted tubule-
Fluid enters at ~25 mL/min because 80% has been reabsorbed. Channels permit Na and Cl reabsorption and little water.
The Collecting duct-
By the time the fluid reaches the end of the DCT 90-95% of the water and solutes have been reabsorbed and returned to the bloodstream.
26. 26 Hormonal regulation-
Renin- Angiotensin -Aldosterone System-
When blood volume and pressure decreases the walls of the arterioles are stretched less and the juxtaglomerular cells, via sympathetic stimulation, secrete the enzyme renin.
Renin stimulates the formation of a amino acid peptide called angiotensin I from angiotensinogen, synthesized in the liver.
Angiotensin I is converted to angiotensin II which is the active hormone.
27. 27 Angiotensin II affects renal physiology 4 ways:
It decreases the GFR by causing vasoconstriction of the afferent arterioles.
It enhances reabsorption of Na, Cl and H2O in the PCT by stimulating the activity of Na/H+ antiporters.
It stimulates the adrenal cortex to release aldosterone, which stimulates the collecting ducts to reabsorb more Na and Cl which increases blood volume.
It stimulates the release of ADH which increases the reabsorption of H2O in the collecting ducts.
28. 28 Antidiuretic hormone (ADH, vasopressin)-
Increases water permeability of vessel
When ADH secretion is maximal urine is extremely concentrated. Works on a negative feedback system.
Atial Natriuetic Peptide (ANP)-
a large increase in blood volume promotes the release of ANP. Suppresses the secretion of Aldosterone and ADH.
Parathyroid hormone-
PTH acts on the PCT to increase phosphate excretion.
Acts on the DCT to increase calcium reabsorbtion.
29. 29 Homeostasis of body fluid volume depends on a large part on the ability of the kidneys to regulate the rate of water loss in urine.
Normal functioning kidneys produce a large volume of dilute urine when fluid intake is excessive and a small volume when fluid intake is low.
ADH controls whether dilute or concentrated urine is formed.
In absence of ADH urine is diluted and contains a high ratio of water in solutes.
In presence of ADH urine is concentrated and the ratio of water to solutes is much lower.
30. 30 Diuretics-
Substances that slow renal reabsorption and cause an elevated urine flow.
Naturally occurring diuretics are caffeine in coffee, tea and soda which inhibit Na reabsorption.
Alcohol in beer, wine and drinks inhibit secretion of ADH.
LOH diuretics like Lasix selectively inhibit Na, K, and Cl.
Thiazide diuretics act in the DCT and promote loss of Na.
31. 31 The increased Na reabsorption from diuretics often causes K secretion and an excessive loss of K in urine. K sparring diuretics can counteract this effect.
Evaluation of Kidney function-
Urinalysis- analysis of volume, physical, chemical and microscopic properties of urine.
Table 23.2 p 919.
Blood tests
Blood Urea Nitrogen (BUN)- measures blood nitrogen that is part of urea. When GFR decreases severely as in renal disease or obstruction, BUN rises steeply.
Plasma creatinine- a level of ^1.5 mg/dL, indicate poor renal function.
32. 32 Renal Plasma clearance- volume of blood that is cleaned of a substance per unit of time. High renal plasma indicates efficient excretion of a substance in urine.
In drug therapy it is important to know a drug�s clearance to determine the correct dosage.
If clearance is high the dosage must also be high and given several times/day to maintain therapeutic levels. Ie- PCN
Dialysis- Artificial cleansing of blood due to renal failure.
Hemodialysis- directly filters patient�s blood.
Continuous ambulatory peritoneal dialysis- uses the peritoneal cavity as the dialysis membrane.
33. 33 A catheter is surgically placed in the peritoneal cavity and connected to a sterile solution which flows into the peritoneal cavity via gravity. The fluid remains in the cavity until waste products diffuse into the solution. It is then drained by gravity in a sterile bag.
Urine drains through the papillary ducts into the minor calyces to unite to form the renal pelvis. Urine then drains via the ureters into the urinary bladder. Discharged from the body via the urethra.
Urinary bladder
Hollow, distensible, muscular organ in the pelvic cavity posterior to the pubic symphysis.
34. 34 Trigone- Small triangular area in the floor of the bladder.
2 urethral openings in the posterior trigone.
1 urethral opening in the anterior portion.
Detrusor muscle
Micturition reflex-
When a volume of urine exceeds 200-400 mL pressure within th bladder increases and receptors in walls transmit nerve impulses via S2 and 3 to trigger a reflex.
Causes contraction of the detrusor muscle and relaxation of the internal urethral sphincter muscle.
Urethra- Small tube from the urethral orifice to the exterior of the body. Terminal portion of the urinary system.
35. 35 Homeostatic imbalances
Glomerulonephritis
nephrotic syndrome
Renal failure
acute renal failure
Chronic renal failure
Renal calculi (Kidney Stones)
Urinary incontinence
36. 36 THAT�S ALL SHE WROTE