Download
1 / 18
270 likes | 1.29k Views
Neuroblastoma. TUMOR BORD. History. 10 month old male. Previously healthy. The history started 1 month before admission. Patient developed fever ,on-off, documented 39 C relieved by antipyretics, with no history of sweating, no rigor. History of poor feeding and decreased activity.

E N D
Neuroblastoma TUMOR BORD
History • 10 month old male. • Previously healthy. • The history started 1 month before admission. • Patient developed fever ,on-off, documented 39 C relieved by antipyretics, with no history of sweating, no rigor. • History of poor feeding and decreased activity. • 2 weeks before admission,the mother noticed that her baby had left upper eyelid swelling. • The swelling increased in size and then the baby could not open his left eye.
She seek medical advise at many peripheral centers in west bank, then she was referred to al-makassed hospital. • In the hospital the baby was found to had abdominal mass. • Abdominal u/s and then CT scan was done which showed abdominal mass originated from suprarenal gland suspected to be neuroblastoma. • FNA biopsy was taken from the mass and the diagnosis was neuroblastoma. • The patient HB was 6 and he received PRBC.
No history of vomitting,no history of diarrhea, no skin rash, no change in urine amount or colour,no abnormal movement, no weight loss. • Developmental history: up to age. • Vaccination history : up to date according to the Palestinian national vaccination program. • Past- medical history and family are not significant.
Examination • Vital signs: -Temp.:37.1C axillary. - HR: 140 beat/m. - RR: 25 breath/m. - B.P. 150/110. -O2 : 98%. • Growth parameters: - Wt.:8.5 kg - Length: 71CM -Head circumference: 46 CM.
Growth chart: • Wt./age:10th.percentile • Length/age: 25th percentile. • Head circumference/age: 50th percentile. General appearance: • Conscious,allert,pale,active,left eyelid swelling which cover eye and eye ball cannot seen. • No palpable LAP. • No skin rash. ENT: free. Chest and heart: free.
Abdomen • Distended, inverted umbilicus, visible veins. • Palpable mass can be felt on the left lumbar area, not attached to skin, not mobile,hard,smooth,ill defined edges ,10x5cm ,upper border cannot be palpated liver and spleen are not palpable. • The mass is dull by percussion. • Neurological examination: free.
Investigations • CBC: -HB:7.5 - WBC:9.7 -N.63% - L.25% • CRP:164 -ESR:64 -LDH:3500 • KFT : NL • LFT :NL • 24 hour urine collection: -Catecholamines:55 - VMA:3.5 -metanephrine:0.2 (all are NL) • bone marrow aspiration and biopsy: Metastatic neuroblastoma.
Bone scan: Increased uptake on skull, sternum and right greater trochanter and distal end of femur. • MIBG scan: - Multiple active lesions on skull, chest and abdomen consistent with neuroblastoma. - Left upper abdomen diffuse mass. • CT scan chest and brain. • CT scan abdomen which was done in al-makassid hospital was reviewed in our hospital.
Treatment • Tumor lyses precaution: -IV fluid 1.5 maintenance+NAHCO3 40meq/litre. -Allopurinol po. • Antihypertensive medications: according to the advise of pediatric nephrologist) - Propronolol po. - Furosemide IV. • Chemotherapy according to protocol.
Neuroblastoma • Embryonic cancer of the peripheral sympathetic nervous system with heterogeneous clinical presentation and course. Epidemilogy: • Third most common pediatric cancer. • 8% of childhood malignancies. • Most common neoplasm in infants.. • 28%-39% of neonatal malignancies. • 90% of cases are diagnosed by 5 yr. of age. • Incidence is slightly higher in boys and in whites.
Pathology • Variable degrees of neural differentiation, ranging from undifferentiated small round cells to mature ganglion cells (ganglioneuroblastoma or ganglioneuroma) • The tumor may resemble other small round cell tumors such as rhabdomyosarcoma ,Ewing sarcoma, and non-Hodgkin lymphoma. Genetics: • Prognostic importance. • Amplification of MYCN is strongly associated with advanced tumor stage and poor outcome independent of stage and age. • Hyperdiploidy confers better prognosis if the child is younger than 1 year of age at diagnosis.
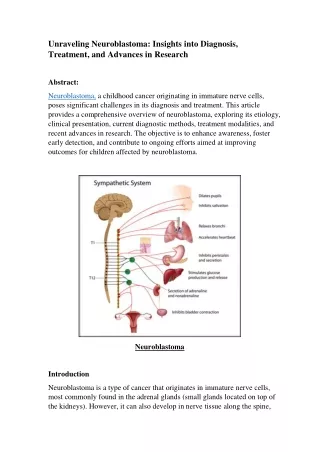
Clinical manifestations • May develop at any site of sympathetic nervous system tissue. • Most cases arise in the abdomen either in the adrenal gland or in retroperitoneal sympathetic ganglia. • Firm nodular mass palpable in the flank or midline causing abdominal discomfort. • Originates from cervical ,thoracic, or pelvic ganglia in 30% of cases. • Metastatic disease can be associated with fever,irritability,FTT,bone pain, orbital proptosis ,and periorbital echymosis.
Metastasis: long bones and skull ,BM ,liver ,lymph nodes and skin. lung mets are rare. • Horner syndrome if location in sup. Cervical ganglion. • Spinal cord or nerve root compression if invade the neural foramina. • Opsomyoclonus. • Increased sweating and hypertension by producing catecholamines. • Secretory diarrhea by VIP.
Diagnosis • Mass or multiple masses on plain radiograph ,CT or MRI. • HVA and VMA are elevated in 95% of cases. • Pathological diagnosis by biopsy. • Cytogenetic. • NB can be diagnosed without tumor biopsy if neuroblasts are observed in BM and elevated HVA and VMA in urine. • Evaluation of metastatic disease should include BM aspirate and biopsies ,bone scan and MIBG scan.
Treatment • Depends on age of patient at diagnosis ,stage of disease ,MYCN STATUS and shimada histology. • Low risk NB : surgery for stage1 and 2 and observation for stage4S . • Intermediate risk NB : surgery , chemotherapy and in some cases radiation therapy. • High risk NB :induction chemotherapy to achieve complete response or very good partial response , with partial response ,resection of the primary tumor followed by focal radiation to the residual tumor. induction is then followed by high dose chemotherapy and autologous stem cell transplantation.