Download
1 / 1
10 likes | 192 Views
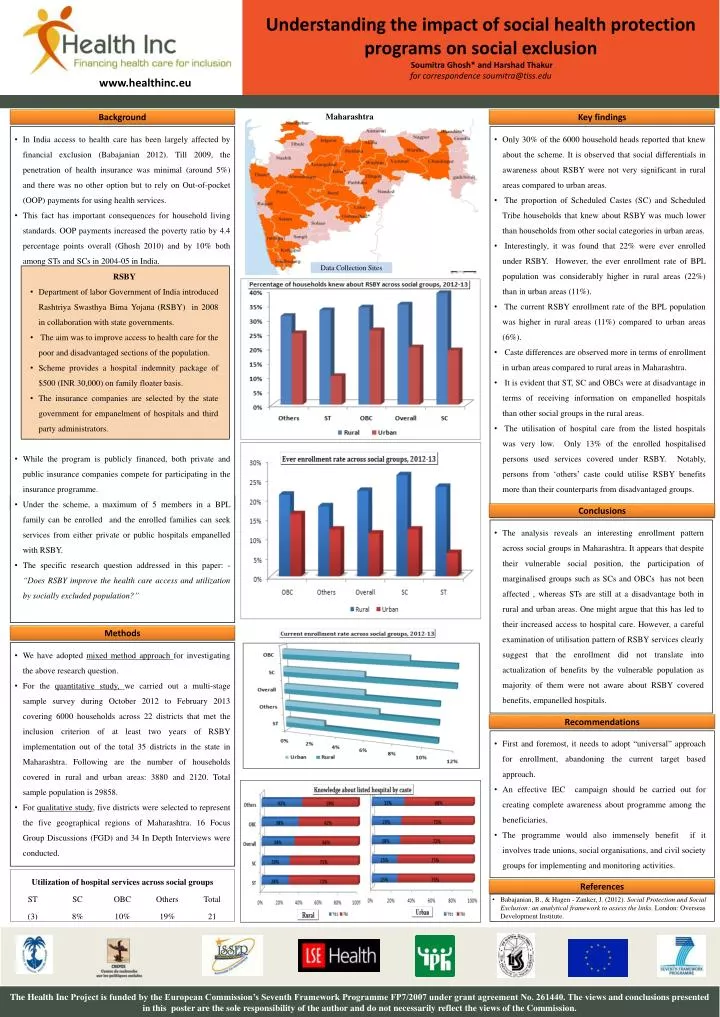
Understanding the impact of social health protection programs on social exclusion Soumitra Ghosh* and Harshad Thakur for correspondence soumitra@tiss.edu. www.healthinc.eu. Background . Maharashtra. Key findings .

E N D
Understanding the impact of social health protection programs on social exclusion Soumitra Ghosh* and Harshad Thakurfor correspondence soumitra@tiss.edu www.healthinc.eu Background Maharashtra Key findings • In India access to health care has been largely affected by financial exclusion (Babajanian 2012). Till 2009, the penetration of health insurance was minimal (around 5%) and there was no other option but to rely on Out-of-pocket (OOP) payments for using health services. • This fact has important consequences for household living standards. OOP payments increased the poverty ratio by 4.4 percentage points overall (Ghosh 2010) and by 10% both among STs and SCs in 2004-05 in India. • While the program is publicly financed, both private and public insurance companies compete for participating in the insurance programme. • Under the scheme, a maximum of 5 members in a BPL family can be enrolled and the enrolled families can seek services from either private or public hospitals empanelled with RSBY. • The specific research question addressed in this paper: - “Does RSBY improve the health care access and utilization by socially excluded population?” • Only 30% of the 6000 household heads reported that knew about the scheme. It is observed that social differentials in awareness about RSBY were not very significant in rural areas compared to urban areas. • The proportion of Scheduled Castes (SC) and Scheduled Tribe households that knew about RSBY was much lower than households from other social categories in urban areas. • Interestingly, it was found that 22% were ever enrolled under RSBY. However, the ever enrollment rate of BPL population was considerably higher in rural areas (22%) than in urban areas (11%). • The current RSBY enrollment rate of the BPL population was higher in rural areas (11%) compared to urban areas (6%). • Caste differences are observed more in terms of enrollment in urban areas compared to rural areas in Maharashtra. • It is evident that ST, SC and OBCs were at disadvantage in terms of receiving information on empanelled hospitals than other social groups in the rural areas. • The utilisation of hospital care from the listed hospitals was very low. Only 13% of the enrolled hospitalised persons used services covered under RSBY. Notably, persons from ‘others’ caste could utilise RSBY benefits more than their counterparts from disadvantaged groups. Data Collection Sites • RSBY • Department of labor Government of India introduced Rashtriya Swasthya Bima Yojana (RSBY) in 2008 in collaboration with state governments. • The aim was to improve access to health care for the poor and disadvantaged sections of the population. • Scheme provides a hospital indemnity package of $500 (INR 30,000) on family floater basis. • The insurance companies are selected by the state government for empanelment of hospitals and third party administrators. Methods Conclusions • The analysis reveals an interesting enrollment pattern across social groups in Maharashtra. It appears that despite their vulnerable social position, the participation of marginalised groups such as SCs and OBCs has not been affected , whereas STs are still at a disadvantage both in rural and urban areas. One might argue that this has led to their increased access to hospital care. However, a careful examination of utilisation pattern of RSBY services clearly suggest that the enrollment did not translate into actualization of benefits by the vulnerable population as majority of them were not aware about RSBY covered benefits, empanelled hospitals. Methods • We have adopted mixed method approach for investigating the above research question. • For the quantitative study, we carried out a multi-stage sample survey during October 2012 to February 2013 covering 6000 households across 22 districts that met the inclusion criterion of at least two years of RSBY implementation out of the total 35 districts in the state in Maharashtra. Following are the number of households covered in rural and urban areas: 3880 and 2120. Total sample population is 29858. • For qualitative study, five districts were selected to represent the five geographical regions of Maharashtra. 16 Focus Group Discussions (FGD) and 34 In Depth Interviews were conducted. Recommendations • First and foremost, it needs to adopt “universal” approach for enrollment, abandoning the current target based approach. • An effective IEC campaign should be carried out for creating complete awareness about programme among the beneficiaries. • The programme would also immensely benefit if it involves trade unions, social organisations, and civil society groups for implementing and monitoring activities. References • Babajanian, B., & Hagen - Zanker, J. (2012). Social Protection and Social Exclusion: an analytical framework to assess the links. London: Overseas Development Institute. The Health Inc Project is funded by the European Commission’s Seventh Framework Programme FP7/2007 under grant agreement No. 261440. The views and conclusions presented in this poster are the sole responsibility of the author and do not necessarily reflect the views of the Commission.