Download
1 / 30
300 likes | 456 Views
Guidelines for Weaning From Short-Term Ventilation. Patients are often intubated electively for surgical or other procedures , or more urgently owing to respiratory distress related to underlying pulmonary disease or traumatic injury .

E N D
Patients are often intubated electively for surgical or other procedures, or more urgently owing to respiratory distress related to underlying pulmonary disease or traumatic injury. • The other common reason for intubation is the need for airway protection because of airway swelling (e.g., as a result of acute inhalation injury) or significant change in mental status (e.g., as with cerebrovascular accident [CVA] or headinjury). • Once the procedure is completed or the patient is stabilized, the goal should be extubation as soon as the patient is able to protect the airway. • The weaning process in this setting may proceed rapidly, based on individual patient response to reducing ventilatory support.
ReadinessCriteria ■ Hemodynamically stable, adequately resuscitated, and not requiringvasoactive support ■ SaO2 >92% on FiO2 ≤40%, positive end-expiratory pressure (PEEP) ≤5 cm H2O ■ Chest x-ray reviewed for correctable factors; treated as indicated ■ Metabolic indicators (serum pH, major electrolytes) withinnormal range ■ Hematocrit >25% ■ Coretemperature >36°C and <39°C ■ Adequate management of pain/anxiety/agitation ■ No residualneuromuscular blockade ■ Arterial blood gases (ABGs) normalized or at patient’s baseline
Weaning Intervention ■ Reduce ventilator rate, then convert to pressure-support ventilation (PSV) only. ■ Wean PSV as tolerated to ≤10 cm H2O. • If patient meets tolerance criteria for at least 2 hours on this level of support and meets extubation criteria ,may extubate. ■ If patient fails tolerance criteria, increase PSV or add ventilator rate as needed to achieve “rest” settings (consistent respiratory rate <20 breaths/minute) and review weaning criteria for correctable factors. ■ Repeat wean attempt on PSV 10 cm after rest period (minimum 2 hours). If patient fails second wean trial, return to rest settings and use “long-term” ventilation weaningapproach.
Tolerance Criteria • If the patient displays any of the following, the weaning trial should be stopped and the patient returned to “rest” settings. ■ Sustained respiratory rate greater than 35 breaths/ minute ■ SaO2 <90% ■ Tidalvolume ≤5 mL/kg ■ Sustainedminute ventilation >200 mL/kg/minute ■ Evidence of respiratory or hemodynamic distress: Laboredrespiratorypattern Increased anxiety, diaphoresis, or both Sustained heart rate >20% higher or lower than baseline Systolic blood pressure >180 mm Hg or <90 mm Hg
ExtubationCriteria ■ Mental status: alert and able to respond to commands ■ Good cough and gag reflex, able to protect airway and clearsecretions ■ Able to move air around endotracheal tube with cuff deflated and end of tube occluded
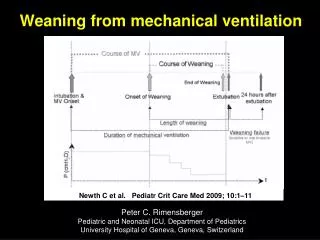
Guidelines for Weaning From Long-Term Ventilation • Patients on mechanical ventilation for longer than 72 hours or those having failed short-term weaning often display significant deconditioningas a result of acute or chronic complex illness, or both. • These patients usually require a period of “exercising” respiratory muscles to regain the strength and endurance needed for successful return to spontaneous breathing. • Goals for this process are: ■ To have the patient tolerate two to three daily weaning trials of reduction in ventilatory support without exercising to the point of exhaustion ■ To rest the patient between weaning trials and overnight on ventilator settings that provide diaphragmatic rest, with minimal or no work of breathing for the patient
ReadinessCriteria ■ Same as for short-term ventilation, with emphasis on hemodynamic stability, adequate analgesia/ sedation (record scores on flow sheet), and normalizing volumestatus
Weaning Intervention ■ Transfer to pressure-support ventilation (PSV) mode, adjust support level to maintain patient’s respiratory rate at less than 35 breaths/minute. ■ Observe for 30 minutes for signs of early failure (same tolerance criteria as with short-term ventilation ■ If tolerated, continue trial for 2 hours, then return patient to “rest” settings by adding ventilator breaths or increasing PSV to achieve a total respiratory rate of less than 20 breaths/minute. ■ After at least 2 hours of rest, repeat trial for 2 to 4 hours at same PSV level as previous trial. If the patient exceeds the tolerance criteria ,stop the trial and return to “rest” settings. In this case, the next trial should be performed at a higher support level than the “failed” trial. ■ Record the results of each weaning episode, including specific parameters and the time frame if “failure” observed, on the bedside flow sheet.
The goal is to increase the length of the trials and reduce the PSV level needed on an incremental basis. • With each successive trial, the PSV level may be decreased by 2 to 4 cm H2O, the time interval may be increased by 1 to 2 hours, or both, while keeping the patient within tolerance parameters. • The pace of weaning is patient-specific and tolerance may vary from day to day. • Review readiness criteria for correctable factors daily and each time the patient “fails” a weaning trial. ■ Ensure nocturnal ventilation at “rest” settings (with a respiratory rate of <20 breaths/minute) for at least 6 hours each night until the patient’s weaning trials demonstrate readiness to discontinue ventilatory support.
DiscontinuingMechanical Ventilation • The patient should be weaned until ventilator settings are FIO2 ≤40%, PSV ≤10 cm H2O, and positive end-expiratory pressure (PEEP) ≤8 cm H2O. • Once these settings are well tolerated, the patient should be placed on continuous positive airway pressure (CPAP) 5 cm H2O or (if tracheostomyin place) on tracheostomy collar. • If the patient meets tolerance criteria over the first 5 minutes, the trial should be continued for 1 to 2 hours. If clinical observation and arterial blood gases (ABGs) indicate that the patient is maintaining adequate ventilation and oxygenation on this “minimal” support, the following options should be considered:
If the patient meets extubationcriteria this step should be attempted. ■ If the patient is on tracheostomy collar, the trials should be continued two to three times per day with daily increases in time on tracheostomy collar by 1 to 2 hours per trial until total time off the ventilator reaches 18 hours per day. • At this point, the patient may be ready to remain on tracheostomy collar for longer than 25 hours unless the tolerance criteriaare exceeded. ■ Ventilator weaning is considered successful once the patient achieves spontaneous ventilation (extubatedor on tracheostomy collar) for at least 25 hours.
METHODS FOR VENTILATOR WEANING • Various methods have been studied for weaning from the ventilator. • Controversies exist over which methods are best. • Some of the most common weaning methods include T-piece or CPAP trials and a gradual PSV reduction. • Comprehensive assessment of the patient’s needs and progress toward weaning, monitoring of the weaning parameters, and following established goals promote successful weaning. • Multidisciplinaryand comprehensiveapproaches to weaning based on a health care professional (nurse) monitoring and promoting a weaning plan with continuity have demonstrated positive outcomes
T-piece Trial • The T-piece is connected to the patient at the desired • FIO2 (usually slightly higher than the previous ventilator setting). • The patient’s response to and tolerance of the trial are continuously observed. • The duration of T-piece trials is not standardized, and some clinicians extubateif an initial trial of 30 minutes ends with acceptable ABGs and patient response. • Some use trials of increasing frequency and duration to evaluate and build the patient’s endurance with periods of rest on the ventilator between trials. • When the latter method is used, the patient is usually deemed ready to be extubated after 25 successive hourson a T-piece.
Synchronized IntermittentMandatory Ventilation Method • The SIMV mode was initially heralded as the optimal weaning mode, allowing for some spontaneous breathing (to prevent respiratory muscle atrophy) while providing a backup rate. • Weaning with the SIMV method entails a gradual reduction in the number of delivered breaths until a low rate is reached (usually 4 breaths/minute). • The patient is then extubated if all other weaning criteria are met. • However, low levels of SIMV (fewer than 4 breaths/minute) may result in a high level of work and fatigue.
Synchronized IntermittentMandatory Ventilation Method • SIMV plus PSV may be used to decrease the work of breathing associated with spontaneous breaths. • It has been suggested that using the combined modes may result in prolonged weaning duration. • As a result, PSV “standalone” mode is often preferred for weaning trials.
Continuous Positive Airway Pressure Method • CPAP entails breathing through the ventilator circuit with a small amount (or zero amount) of positive pressure. • The use of CPAP versus the use of a T-piece for weaning is controversial. • Often the decision to use one over the other is determined by observing the patient’s response, or is simply based on the clinician’s preference.
Pressure-Support Ventilation Method • Low levels of PSV decrease the work of breathing associated with endotracheal tubes and ventilator circuits. • Weaning using the PSV mode entails a progressive decrease in pressure based on the patient maintaining an adequate tidal volume (8 to 12 mL/kg) and a respiratory rate of less than 25 breaths/minute. • PSV is associated with less work of breathing than with volume modes, so longer weaning trialsmay be tolerated.
ADJUNCTS TO WEANING • Several adjuncts to long-term weaning are used to improve weaning tolerance and patient comfort. • The fenestrated tracheostomy tube provides for communication during weaning periods, improving patient interaction. • The fenestrated tracheostomytube has an opening in the outer cannulabut not the inner cannula. • With the inner cannula in place and the cuff inflated, the patient is easily mechanically ventilated.
ADJUNCTS TO WEANING • During the weaning process, the inner cannula is removed, the cuff deflated, the outer cannula capped, and supplemental oxygen supplied by nasal cannula. • This system permits air to pass the vocal cords, allowing verbal communication by the patient.
The cuff should never be inflated while the inner cannula is capped because the patient will be unable to breathe. • The Kirshner button or Shileyspeaking valve provides communication during weaning periods for patients with tracheostomy tubes. • These provide less resistance than the fenestrated tracheostomy tube, and with the Shileyvalve, supplemental oxygen can be given through a side port. • Humidified air with a tracheostomy collar may be required to keep the airway moist and prevent secretions from drying. Use of a large endotracheal tube (>7.0 mm)
decreases resistance to breathing and decreases the work of breathing. • A larger endotracheal tube also supports bronchoscopyto remove secretions when needed. • Tracheostomy in many instances is more comfortable for patients and allows for improved oral care,and improved communication
EXTUBATION CRITERIA • Whichever mode or combination of modes is used for weaning, extubation cannot occur until several criteria are met based on short-term or long-term ventilation • Before extubation, the patient must be able to maintain his or her own airway, as evidenced by an appropriate level of consciousness and the presence of cough and gag reflexes. • In all patients, but especially in those with a history of difficult intubation or reactive airway disease, the “cuff leak test” should be performed before extubation.
EXTUBATION CRITERIA • This entails deflation of the tube cuff (after suctioning of the oropharynx) and a brief period of occluding the endotracheal tube to demonstrate an air leak with patient inspiration. • Absence of a leak can indicate edema, and may predict laryngeal stridorpostextubation. If the cuff leak test fails, the patient may be given corticosteroids to reduce edema for 25 to 48 hours, then reassessed for cuff leak. • Direct visualization of the trachea with a bronchoscope may be obtained before extubation to determine if the edema has resolved.
EXTUBATION CRITERIA • Extubation should never occur unless a qualified person is available to reintubate emergently if the patient does not tolerate extubation. • After explaining the procedure and preparing the patient, the nurse suctions the patient’s tube and posterior oropharynx. • Equipment includes an MRB and mask at bedside. • After the nurse loosens the endotracheal tube securing device or tape, the cuff is deflated. • The endotracheal tube is removed quickly while having the patient cough. • The patient’s mouth is suctioned and humidified oxygen is applied immediately.
EXTUBATION CRITERIA • The patient is evaluated for immediate signs of distress: stridor, dyspnea, and decrease in SaO2. • Treatment for stridor includes inhaled epinephrine and sometimes administration of intravenous steroids (because steroids do not work immediately, they are given before extubation in those at risk). • If these interventions fail, immediate re-intubation may be necessary.