Download
1 / 1
10 likes | 137 Views
CONTINUOUS GLUCOSE MONITORING, ORAL GLUCOSE TOLERANCE, AND INSULIN – GLUCOSE PARAMETERS IN ADOLESCENTS WITH SIMPLE OBESITY Soliman A, El Awwa A. Adel A, Yassin M, Department of Pediatrics, Hamad Medical Center, Doha P O Box 3050, Doha, Qatar. Introduction.

E N D
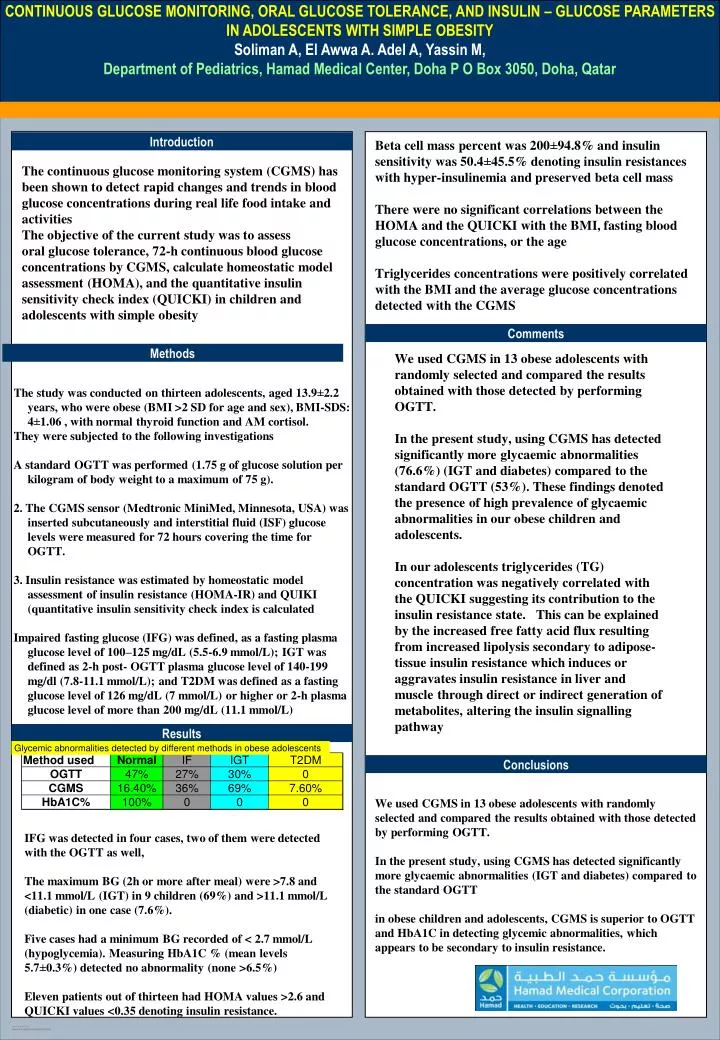
CONTINUOUS GLUCOSE MONITORING, ORAL GLUCOSE TOLERANCE, AND INSULIN – GLUCOSE PARAMETERS IN ADOLESCENTS WITH SIMPLE OBESITY Soliman A, El Awwa A. Adel A, Yassin M, Department of Pediatrics, Hamad Medical Center, Doha P O Box 3050, Doha, Qatar Introduction Beta cell mass percent was 200±94.8% and insulin sensitivity was 50.4±45.5% denoting insulin resistances with hyper-insulinemia and preserved beta cell mass There were no significant correlations between the HOMA and the QUICKI with the BMI, fasting blood glucose concentrations, or the age Triglycerides concentrations were positively correlated with the BMI and the average glucose concentrations detected with the CGMS The continuous glucose monitoring system (CGMS) has been shown to detect rapid changes and trends in blood glucose concentrations during real life food intake and activities The objective of the current study was to assess oral glucose tolerance, 72-h continuous blood glucose concentrations by CGMS, calculate homeostatic model assessment (HOMA), and the quantitative insulin sensitivity check index (QUICKI) in children and adolescents with simple obesity Comments Methods We used CGMS in 13 obese adolescents with randomly selected and compared the results obtained with those detected by performing OGTT. In the present study, using CGMS has detected significantly more glycaemic abnormalities (76.6%) (IGT and diabetes) compared to the standard OGTT (53%). These findings denoted the presence of high prevalence of glycaemic abnormalities in our obese children and adolescents. In our adolescents triglycerides (TG) concentration was negatively correlated with the QUICKI suggesting its contribution to the insulin resistance state. This can be explained by the increased free fatty acid flux resulting from increased lipolysis secondary to adipose-tissue insulin resistance which induces or aggravates insulin resistance in liver and muscle through direct or indirect generation of metabolites, altering the insulin signalling pathway The study was conducted on thirteen adolescents, aged 13.9±2.2 years, who were obese (BMI >2 SD for age and sex), BMI-SDS: 4±1.06 , with normal thyroid function and AM cortisol. They were subjected to the following investigations A standard OGTT was performed (1.75 g of glucose solution per kilogram of body weight to a maximum of 75 g). 2. The CGMS sensor (Medtronic MiniMed, Minnesota, USA) was inserted subcutaneously and interstitial fluid (ISF) glucose levels were measured for 72 hours covering the time for OGTT. 3. Insulin resistance was estimated by homeostatic model assessment of insulin resistance (HOMA-IR) and QUIKI (quantitative insulin sensitivity check index is calculated Impaired fasting glucose (IFG) was defined, as a fasting plasma glucose level of 100–125 mg/dL (5.5-6.9 mmol/L); IGT was defined as 2-h post- OGTT plasma glucose level of 140-199 mg/dl (7.8-11.1 mmol/L); and T2DM was defined as a fasting glucose level of 126 mg/dL (7 mmol/L) or higher or 2-h plasma glucose level of more than 200 mg/dL (11.1 mmol/L) Results Conclusions We used CGMS in 13 obese adolescents with randomly selected and compared the results obtained with those detected by performing OGTT. In the present study, using CGMS has detected significantly more glycaemic abnormalities (IGT and diabetes) compared to the standard OGTT in obese children and adolescents, CGMS is superior to OGTT and HbA1C in detecting glycemic abnormalities, which appears to be secondary to insulin resistance. IFG was detected in four cases, two of them were detected with the OGTT as well, The maximum BG (2h or more after meal) were >7.8 and <11.1 mmol/L (IGT) in 9 children (69%) and >11.1 mmol/L (diabetic) in one case (7.6%). Five cases had a minimum BG recorded of < 2.7 mmol/L (hypoglycemia). Measuring HbA1C % (mean levels 5.7±0.3%) detected no abnormality (none >6.5%) Eleven patients out of thirteen had HOMA values >2.6 and QUICKI values <0.35 denoting insulin resistance.






