Download
1 / 43
430 likes | 545 Views
Expanded Criteria Deceased Donors: The US Perspective. Donald E. Hricik, M.D. University Hospitals Case Medical Center Case Western ReserveUniversity Post-graduate Education Director American Society of Transplantation Cleveland, Ohio USA. The “good” news.

E N D
Expanded Criteria Deceased Donors:The US Perspective Donald E. Hricik, M.D. University Hospitals Case Medical Center Case Western ReserveUniversity Post-graduate Education Director American Society of Transplantation Cleveland, Ohio USA
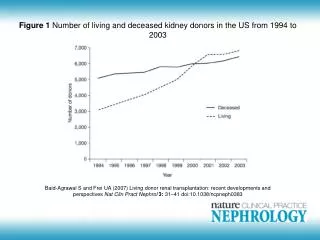
There has been an increase in kidney transplant numbers… Total number of transplants by year
Cadaveric Renal Allograft Survival • Radiation • Prednisone • 6-MP • Cyclosporine Emulsion • Tacrolimus Cyclosporine • MMF • OKT3 • Dicluzimab • Basiliximab • AZA • Thymoglobulin • Sirolimus • ATGAM ‘60 ‘65 ‘70 ‘75 ‘80 ‘85 ‘90 ‘95 ‘00 Year Adapted from Stewart F, Organ Transplantation, 1999
The number of people living with a functioning kidney transplant doubled between 1995 and 2004
Dialysis vs Transplantation Waiting-list dialysis Waiting-list dialysis Transplant Transplant Projected Years of Life Diabetes Glomerulo- nephritis Other P<0.001 Wolfe RA et al. N Engl J Med. 1999;341:1725-1730.
Trends in Kidney Transplantation(US 1995-2005) The Organ Procurement and Transplantation Network (OPTN). www.optn.org. 2006.
Current and projected waitlist for deceased donor kidneys • As of May 2003 54,000 awaiting CRT • Projected waitlist 95,550 in 2010 (Xue et al. JASN12:2753,2001) • Approx 9,000 CRTs per annum
Mortality on Waiting List Ojo AO et al. 2001 Merion RM et al. 2005 Annual Death Rate on Waiting List (%) HTN=hypertension; DM=diabetes mellitus. Ojo AO et al. J Am Soc Nephrol. 2001;12:589. Merion RM et al. JAMA. 2005;294:2726-2733.
Allograft Survival:Impact of Donor Source and Waiting Time Cadaveric Living 100 100 90 90 80 80 70 70 Event-free graft survival (%) 60 60 50 50 Preemptive 0-6 months 6-12 months 12-24 months >24 months Preemptive 0-6 months 6-12 months 12-24 months >24 months 40 40 30 30 20 20 0 12 24 36 48 60 72 84 96 108 120 0 12 24 36 48 60 72 84 96 108 120 Months Posttransplant Months Posttransplant Meier-Kriesche HU, Kaplan B. Transplantation. 2002;74:1377-1381.
US Kidney Transplants by Donor Type The Organ Procurement and Transplantation Network (OPTN). www.optn.org. 2006.
29.4 2,198 18.7 3,584 18.5 2,803 18.0 3,094 10.2 34,208 Living donor tx is the Best Solution 1998-2002 UNOS 100 79 80 68 67 60 66 48 40 Graft Survival Source n t1/2 30 HLA-Id 1-Haplo 20 Spouse Unrelated p<0.001 Deceased 10 0 1 2 3 4 5 6 7 8 9 10 Years Posttransplant Cecka, Clinical Transplants 2003 (p.4)
Initiatives Designed to Increase the Pool of Deceased Donor Organs • Expanded Criteria Donors (ECD) • Donors After Cardiac Death (DCD) (non-heartbeating deceased donors)
“Expanded Criteria” DonorsKaufman HM et al Transplant Rev 1997 • “Suboptimal” • “Marginal” • “Inferior” • “Nonstandard
Relative Risk of Graft Loss Based on Donor CharacteristicsPort et al Transplantation 74;1281, 2002 • UNOS data 29,068 first cadaveric transplants 1995-2000 • Donor factors associated with 1.7 increased risk of graft loss -Age < 10 yr or >/= 40 yr -Creatinine > 1.5 mg% (135 uM) -History of hypertension -CVA as cause of death
Relative Risk of Graft Loss Based on Donor CharacteristicsPort et al Transplantation 74;1281, 2002
Survival Benefit from Marginal Kidneys Relative Risk (RR) of Death Days since transplantation (Equal time from wait-listing) Ojo et al. J Am Soc Nephrol 2001; 12: 589.
The UNOS ECD Program • UNOS Kidney Working Group – March 2001 • Recommendations for formal criteria to define ECDs • Policy operational in October 2002 • Goals • Reduce waiting times • Increase the number of transplants performed • Reduce cold ischemia time associated with ECDs
(Expanded) Criteria Yielding a Relative Risk of Graft Failure > 1.7 (compared to reference group) • Age > 60 years • Age > 50 with at least 2 of the following 3: • History of hypertension • CVA as cause of death • Terminal Cr > 1.5 mg/dl
ECD Program in the US • No separate waiting list for ECD kidneys • Patients must provide informed consent • Patients may revoke consent at any time • By July 2003: • 43% of patients on the US waiting list consented for ECD kidneys • Number of ECD kidneys recovered increased by 18% (versus 1 % increase for standard donors) • ECD kidneys with cold ischemia < 12 hours increased from 10% (2001) to 17%
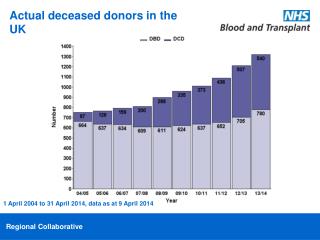
Increase in donors from ECD and DCD Cohen et al, American Journal of Transplantation 2006; 6 (Part 2): 1153–1169
3-Year Graft Survival by Donor Type 6 Mismatch 0 Mismatch 3-Year Graft Survival (%) 3-Year Graft Survival (%) ECD=expanded criteria donor OPTN/SRTR 2005 Annual Report www.ustransplant.org.
Why is outcome worse? • Impaired function with nephron mass • CIT • DGF • Increased immunogenicity • Impaired ability to repair tissue
Delayed graft function is more frequent in ECD and DCD kidneys Cohen et al, American Journal of Transplantation 2006; 6 (Part 2): 1153–1169
Graft Survival (%) by expanded Donor Status* (RR cut point of 1.7) *Adjusted for donor race and sex, recipient: age, race, ethnicity, sex, BMI, primary cause ESRD, time on dialysis, cold ischemia time, pre-transplant transfusion status, PRA, HLA mismatch SRTR
Graft Survival (%) by Relative Risk Categories* *Adjusted for donor race and sex, recipient: age, race, ethnicity, sex, BMI, primary cause ESRD, time on dialysis, cold ischemia time, pre-transplant transfusion status, PRA, HLA mismatch
The Tradeoff Between Waiting Time and Kidney QualitySchnitzler et alTransplantation, 75:1940,2003 • “how much longer will an individual have to wait after refusing a kidney from an ECD before the poorer outcomes and increased costs of waiting on dialysis outweigh the benefits gained from receiving a better standard donor kidney?”
Who Should Receive an ECD kidney ?Gaston et al. Am J Transplant 2003 • The ECD List is usually shorter and thus ECD kidney may offer way to reduce waiting time • Choice relates to balance between life expectancy and waiting time • Approach will depend on local waiting time • In general, ECD kidneys should be directed towards: -Any candidate over 60 years of age -Any diabetic candidate over 40 years of age -Any candidate with failing vascular access -Any candidate whose expected waiting time exceeds their life expectancy
Deceased Donor Allocation According to Net Lifetime Survival Benefit
The argument for changing allocation: The Recipient Perspective 1) The waiting list is growing and a significant proportion of the growth is the elderly 2) Elderly recipients often die with good graft function • Calculations show net gain in “kidney-years” if young kidneys are limited to young patients • Therefore: allocation should be changed to give young kidneys to young recipients.
The argument for changing allocation: The ECD perspective 1) Using ECD donors will increase the number of transplants and shorten waiting time 2) ECD’s are associated with worse outcome 3) Elderly recipients have limited lifespan 4) Therefore: elderly (DCD) donors should be used in elderly recips
Average gain in youngrecipients =27.1 months Average loss in oldrecipients =18.4 months Projected patient survival gain versus loss by not transplanting young donors to old recipients 50 40 30 20 10 0 –10 –20 –30 Net effect on survival (months) 60–64 65–69 70+ 18–29 30–39 40–49 50–59 Recipient age Schold JD et al. Am J Transplant 2006; 6:1689
Who should accept an ECD? In OPO’s with long wait times (>1350 days), ECDs should be offered to patients >40 (decreased mortality vs waiting) In OPO’s with short wait times only recipients with diabetes had a benefit to getting an ECD kidney Merion et al JAMA 2005
What Do Patients Think? Geddes et al, AJKD, 46: 949-956, 2005 University of Glasgow, Scotland 104/153 (68%) dialysis patients and 128/142 (90%) tx recips answered the questionnaire Scenario: A kidney becomes available for 2 patients who have been on dialysis for 3 years: 1 is 20 yrs old, the other 60. All else is equal.
What Do Patients Think? 20 year old - 34.9% 60 year old - 6.9% Age should not matter - 50.4% Do not know - 7.8% 20 yr oldAge should not matter + don’t know < 50 36.7% 56.6% 50-70 25.8% 66.7% >70 55.8% 37.3%
Alternate Measures of Success? Quality of life? How to measure? Is a quality year in a 30 yr old the same as a 60 yr old? Should someone reaching retirement have the opportunity to enjoy their retirement? Is this better or worse than life-enjoyment for a 30 yr old?
Conclusions • ECD kidneys, as used currently, are associated with reduced graft function and long-term graft survival • However, they provide acceptable function in that they offer a significant survival benefit as compared to dialysis • This benefit will be greater for those patients with a shortened lifespan, which increases the adverse effect of waiting • Available data suggest assigning ECD to older/ sicker recipients to ensure optimal risk:benefit
HOWEVER: • Old for old may be detrimental to the elderly! • Dialysis and tx patients are not in favor of favoring young vs old • Kidney-years is not the only measure of success
The REAL Conclusion The reality is that there is still a shortage! “Even in an ideal world in which all brain-dead potential donors became actual donors and the demand for organs remained constant rather than increasing, the supply of organs ….could not meet the needs of all the patients on waiting lists.” Sheehy et al, Estimating the number of potential organ donors in the United States. N Engl J Med. 14: 667-74, 2003