Download
1 / 12
140 likes | 350 Views
“Calcification of Different Designs of Silicone Intraocular Lenses in Eyes with Asteroid Hyalosis” Liliana Werner, MD, PhD Jack Stringham, MS, Bryan Monson, MD, Raymond Theodosis, MS, Nick Mamalis, MD John A. Moran Eye Center, University of Utah, Salt Lake City, UT, USA.

E N D
“Calcification of Different Designs of Silicone Intraocular Lenses in Eyes with Asteroid Hyalosis” Liliana Werner, MD, PhD Jack Stringham, MS, Bryan Monson, MD, Raymond Theodosis, MS, Nick Mamalis, MD John A. Moran Eye Center, University of Utah, Salt Lake City, UT, USA -The authors of this poster have received research funding from Alcon, Allergan, AMO, Bausch & Lomb, Calhoun, Medennium, NuLens, Powervision, Rayner, and Visiogen. -Supported in part by the Research to Prevent Blindness Olga Keith Wiess Scholar Award (Liliana Werner, MD, PhD).
Background In 2004, there were 4 reported cases of calcification of silicone plate intraocular lenses (IOLs) in eyes with asteroid hyalosis.1,2 Later, we reported calcification of an AMO SI-30 lens (three-piece design) in a patient with bilateral asteroid hyalosis; the hydrophobic acrylic lens implanted in the contralateral eye of the patient was not opacified.3 Another report on calcification of a silicone plate lens in asteroid hyalosis was more recently published.4 The deposits on the 6 above-mentioned cases were located on the posterior optic surface of the lenses, and could be partially removed by Nd:YAG laser. However, progressive re-accumulation of deposits on the posterior optic surface of the silicone lenses was observed after the laser procedure (Figure 1). December 99 (post Nd:YAG) June 01 August 98 Figure 1: Case of Dr. James Gills, USA.
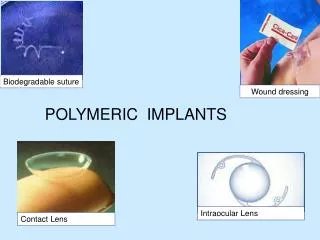
Dystrophic calcification of IOLs requiring explantation has primarily been associated with hydrophilic acrylic designs (Figure 2). With these lenses, the calcified deposits could not be removed with YAG laser application, and were present on the anterior and/or posterior surfaces of the lenses (as well as within the optic substance). Figure 2: Hydrophilic acrylic lenses explanted because of calcification. Since the initial reports on calcification of silicone lenses in eyes with asteroid hyalosis,1-4 we had the opportunity to analyze in our laboratory 16 other silicone lenses of various designs and manufactured from different silicone materials, which were explanted because of optic opacification due to surface deposits. In this study we describe the analyses performed on the 16 silicone explants, as well as the prevalence of asteroid hyalosis in this series, in comparison to a series of hydrophilic acrylic lenses explanted because of calcification.5
All explanted lenses underwent gross and light microscopic analyses with photodocumentation; • Selected lenses were stained with alizarin red for calcium; • Selected lenses underwent scanning electron microscopy (SEM; FEI Nanova 630, OR, USA) coupled with energy dispersive X-ray spectroscopy (EDS; Genesis 5.21 by EDAX, NJ, USA) for analysis of elemental composition of surface deposits; • The clinical data in relation to 111 hydrophilic acrylic lenses explanted because of calcification and analyzed in our laboratory was also assessed for comparison.
Results • Of the 16 newly reported cases, a history of asteroid hyalosis in the corresponding eye was confirmed in 13 (case numbers 1-8, 10-12, 14 and 15). Review of the patient chart in case number 9 showed that the only vitreous notation was posterior vitreous detachment with floaters in both eyes; no notes regarding the presence of asteroid hyalosis were found in patient charts in cases 13 and 16. • The cases shared some common clinical characteristics. The lenses were all explanted because of decrease in visual acuity associated with the presence of whitish deposits on the posterior optic surface (Figure 3). Nd:YAG laser posterior capsulotomy was performed in 12 cases 7.57 +/- 4.21 years after IOL implantation, generally because of a diagnosis of decrease in visual acuity due to posterior capsule opacification. During the same session, the deposits on the posterior optic surface were observed, and could be partially removed or “dusted” from it. However, there was a gradual increase in the density of the deposits after the procedure, mainly within the capsulotomy opening on the posterior surface of the lens.
Dr. J. Gills (SI-40) Dr. U. Reinking (411S) Dr. J. Jones (SI-30; after Nd:YAG) Dr. J. Jones (SI-30; before Nd:YAG) Figure 3: Clinical photographs of 3 cases of opacification of silicone lenses due to surface deposits.
Plate, large holes (RI = 1.413) SI-30 (RI = 1.46) Plate, small holes (RI = 1.413) ClariFlex (RI = 1.46) Z9001 (RI = 1.46) SI-40 (RI = 1.46) LI 61U (RI = 1.429) Gross evaluation of the posterior optic surface of the explanted IOLs revealed a white deposition concentrated in the central 3 mm optic zone of the lens in most cases, with irregular eccentric clearing. The 16 lenses were of 8 designs, from 5 manufacturers, made of 5 different silicone materials (Figure 4). 411 S (RI = 1.430) Figure 4: Gross photographs showing 1 of each of the 8 silicone IOL designs represented in this series (RI = Refractive Index).
Light microscopy demonstrated that the white deposits formed an almost confluent crust in some areas, interspersed with clear areas on the IOL posterior optic surface. Nd:YAG pits corresponding to previous Nd:YAG laser treatment were present on the IOL posterior optic surface in 12 cases. Staining with alizarin red was positive for calcium (cases number 13 and 16). SEM and EDS findings were similar for all lenses undergoing this evaluation (cases 7, 9, 12, and 14). EDS performed on the deposits demonstrated the presence of phosphate (P) and calcium (Ca), in addition to the carbon, oxygen, and silicon peaks (Figure 5). SEM LM LM EDS Figure 5: Light microscopy (LM), SEM and EDS analyses of some of the silicone lenses included in this series.
Regarding the hydrophilic acrylic lenses explanted because of optic opacification, we reviewed 111 cases undergoing pathology analyses in our laboratory. The lenses consisted of 8 different designs, explanted in 12 different countries between 2003 and 2009. All lenses had granules on the optic surface, within the lens substance, or both, consistent with postoperative calcification. A history of asteroid hyalosis in the corresponding eye was not found in any of the cases (Figure 6). Figure 6: Clinical (top) and gross (bottom) photographs from cases of postoperative calcification of different hydrophilic acrylic lenses.
Discussion / Conclusions • Asteroid hyalosis is a vitreous disease characterized by brilliant reflecting particles (asteroid bodies) floating in an apparently normal vitreous body. While their composition and mode of formation remain unclear, it is certain that asteroid bodies are composed of calcium and phosphate.6 • Studies on the barrier function of the posterior capsule demonstrated that it serves as a barrier only to large nonelectrolytes or negative electrolytes (e.g., lipids, proteins, hyaluronic acid, enzymes).7 Therefore, it is not surprising that calcium and phosphate originated from the vitreous in eyes with asteroid hyalosis may cross the posterior capsule and precipitate on the posterior IOL surface. • This study has found no association between asteroid hyalosis and calcification of hydrophilic acrylic lenses (0/111 cases of explantation analyzed in our laboratory or 0.0%). There are now 22 cases of calcification related to 8 different designs of silicone lenses described in the literature, of which 86.4% were in eyes with confirmed asteroid hyalosis.
In light of the increasing number of opacified silicone lenses in eyes with asteroid hyalosis, involving a variety of IOL designs, our findings might be added to the list of pros and cons surgeons consider when selecting or recommending an IOL. References • Foot L, Werner L, Gills JP, et al. Surface calcification of silicone plate intraocular lenses in patients with asteroid hyalosis.Am J Ophthalmol 2004; 137:979-87. • Wackernagel W, Ettinger K, Weitgasser U, et al. Opacification of a silicone intraocular lens caused by calcium deposits on the optic.J Cataract Refract Surg 2004; 30:517-20. • Werner L, Kollarits CR, Mamalis N, Olson RJ. Surface calcification of a three-piece silicone intraocular lens in a patient with asteroid hyalosis: A clinicopathologic case report.Ophthalmology 2005; 112:447-52. • Fuchihata M, Saito Y, Kitaguchi Y, et al. [Calcification on the posterior surface of an implanted silicone intraocular lens in a patient with asteroid hyalosis].Nippon Ganka Gakkai Zasshi 2006; 110:736-40. • Stringham J, Werner L, Monson B, et al. Calcification of different designs of silicone intraocular lenses in eyes with asteroid hyalosis. Ophthalmology 2010 (in press). • Winkler J, Lunsdorf H. Ultrastructure and composition of asteroid bodies.Invest Ophthalmol Vis Sci 2001;42:902-7. • Ozaki L. The barrier function of the posterior capsule.Am Intra-Ocular Implant Soc J 1984; 10:182-4.