Download
1 / 70
890 likes | 1.79k Views
Paraneoplastic syndromes. PRESENTED BY: DR. HITESH GOUR J.R. PULMONARY MEDICINE. DEFINATION. Paraneoplastic syndromes refer to the disorders that accompany benign or malignant tumors but are not directly related to mass effects or invasion by the primary tumor or its metastases.

E N D
Paraneoplastic syndromes PRESENTED BY: DR. HITESH GOUR J.R. PULMONARY MEDICINE
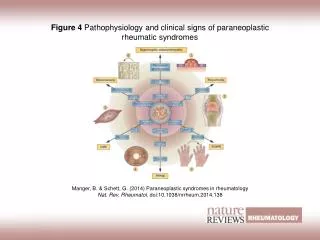
DEFINATION • Paraneoplastic syndromes refer to the disorders that accompany benign or malignant tumors but are not directly related to mass effects or invasion by the primary tumor or its metastases. • Although, almost every type of malignancy has the potential to produce hormones or cytokines or to induce immunologic responses , tumors of neuroendocrine origin, such as small cell lung carcinoma and carcinoids are common causes of paraneoplastic syndromes. • So, atypical clinical manifestations in a patient with cancer should prompt consideration of a paraneoplastic syndrome.
PARANEOPLASTIC SYNDROMES ETIOLOGY: • Ectopic hormones refers to hormone production from an atypical tissue source. • Several molecular mechanisms has been suggested to cause ectopic hormone production, but this process remains incompletely understood. • Genetic rearrangements can explain aberrant hormone expression e.g., translocation of the parathyroid hormone (PTH) gene resulted in high levels of PTH expression in an ovarian carcinoma, because the genetic rearrangement brings the PTH gene under the control of ovary-specific regulatory elements
ectopic expression is typically characterized by abnormal regulation of hormone production (e.g., defective feedback control)that can lead to substantial morbidity and can complicate the cancer treatment plan
Paraneoplasticsundromes associated with bronchogenic carcinoma Endocrine: • Cushing's syndrome • SIADH • Hypercalcemia • Carcinoid syndrome • Hyperglycemia/hypoglycemia • Gynecomastia • Galactorrhea • Growth hormone excess • Calcitonin secretion • Thyroid-stimulating hormone
Neurological • Lambert-Eaton myasthenic syndrome • Peripheral neuropathy • Encephalopathy • Myelopathy • Cerebellar degeneration • Psychosis • Dementia • Cancer related retinopathy • Opsoclonus and myoclonus
MUSCULOSKELETAL • Clubbing • Hypertrophic osteoarthropathy • Polymyositis • Osteomalacia • Myopathy
Cutaneous • Dermatomyositis • Acanthosisnigricans • Pruritus • Erythemamultiforme • Hyperpigmentation • Urticaria • Scleroderma
Vascular/hematologic • Thrombophlebitis • Arterial thrombosis • Granulocytosis • Nonbacterial thrombotic endocarditis • Thrombocytosis • Polycythemia • Hemolyticanemia • Red cell aplasia • Dysproteinemia • Leukemoid reaction • Eosinophilia • Thrombocytopenic purpura
Miscellaneous • Cachexia • Fatigue • Hyperuricemia • Nephrotic syndrome
Ectopic Corticotropin Syndrome • Ectopic production of corticotropin or corticotropin-releasing hormone with associated Cushing's syndrome has been identified in patients who have SCLC, carcinoidtumor (lung, thymus, or pancreas), and neurocresttumors such as pheochromocytoma, neuroblastoma, and medullary carcinoma of the thyroid. • SCLC accounts for 75% of cases, although only 1% to 2% of patients with SCLC develop Cushing's syndrome. Cushing's syndrome is seldom caused by NSCLC
Classic features of Cushing's syndrome include truncal obesity, striae, rounded (moon) facies, dorsocervical fat pad (buffalo hump), myopathy and weakness, osteoporosis, diabetes mellitus, hypertension, and personality changes. • Because of rapid growth of SCLC ,patients are more likely to present with edema, hypertension, and muscular weakness than with the classic features of Cushing's syndrome. • Hypokalemic alkalosis and hyperglycemia are usually present.
Patients with SCLC and Cushing's syndrome have shortened survival compared to those without the syndrome, perhaps because of frequent opportunistic infections. • The best screen for Cushing's syndrome is the 24-hour urine free cortisol measurement. • Elevation of cortisol production, lack of suppression with high-dose dexamethasone, and plasma corticotropin levels greater than 200 pg/mL (40 pmol/L) are highly suggestive of ectopic corticotropin as the cause of Cushing's syndrome in the absence of a pituitary adenoma. The plasma level of corticotropinis elevated in many, but not in all patients.
Treatment: • Adrenal enzyme inhibitors such as metyrapone, aminoglutethimide, and ketoconazole, given alone or in combination. Ketoconazole given orally at a dosage of 400 to 1200 mg/day or metyrapone 250 to 750 mg three times per day control hypercortisolism within a few days to weeks, • Dose adjustments are based on achieving normal urinary free cortisol levels or morning plasma cortisols of 7 to 11 ýg/mL. • Symptomatic hypoadrenalism may result from treatment. • When Cushing's syndrome arises from SCLC, it is advisable to proceed with appropriate chemotherapy and carefully watch for superimposed infections. • Cushing's syndrome related to a bronchial carcinoid or thymiccarcinoid is best treated by surgical resection of the tumor.
Syndrome of Inappropriate Antidiuretic Hormone Secretion • SIADH production defined as low serum and a dilute plasma osmolality along with a higher or “inappropriate” urine osmolality in the presence of continous urinary sodium excreation. • 10% of patients with SCLC exhibit SIADH,.SCLC accounts for approximately 75% of cases of SIADH. • Antidiuretic hormone (vasopressin) is secreted in the anterior hypothalamus and exerts its action on the renal collecting ducts by enhancing the flow of water from the lumen into the medullaryinterstitium, thereby concentrating the urine.
The criteria for the diagnosis of SIADH include (1) hyponatremia associated with serum hypoosmolality (<275 mOsm/kg), (2) inappropriately elevated urine osmolality (>200 mOsm/kg) relative to serum osmolality; (3) elevated urine sodium (>20 mEq/L); (4) clinical euvolemia without edema; and (5) normal renal, adrenal, and thyroid function. • The serum uric acid is usually low, and the urine osmolality–to–serum osmolality ratio is frequently greater than 2. • The severity of symptoms is related to the degree of hyponatremia and the rapidity of the fall in serum sodium.
Symptoms of hyponatremia include anorexia, nausea, and vomiting. With a rapid onset of hyponatremia, symptoms caused by cerebral edema may include irritability, restlessness, personality changes, confusion, coma, seizures, and respiratory arrest.
Treatment: • In minimally symptomatic or asymptomatic patients, fluid restriction of 500 to 1000 mL/24 hr is the initial treatment of choice. • Conivaptan is an intravenous vasopressin receptor antagonist that has been shown to be useful in correcting hyponatremia but its use is limited to the hospital.
If further treatment is needed, oral demeclocycline (900–1200 mg/day) is given. It induces a nephrogenic diabetes insipidus and blocks the action of antidiuretic hormone on the renal tubule, thereby increasing water excretion. • The onset of action varies from a few hours to a few weeks, so this drug is not recommended for acute emergency treatment. • Demeclocycline has potential kidney toxicity. • In patients who have more severe or life-threatening symptoms (serum sodium <115 mEq/L), treatment consists of intravenous saline, supplemental potassium, and diuresis with loop diuretics such as furosemide or ethacrynic acid.
With severe confusion, convulsions, or coma, treatment is with 300 mL of 3% saline given over 3 to 4 hours in combination with a loop diuretic (saline without a diuretic will not increase the sodium concentration). • Rapid correction of the sodium may have life-threatening consequences, and caution is advised. • The rate of correction of the sodium is best limited to a maximum of 20 mEq/L/day, until a level of 120 to 130 mEq/L is reached. • Faster correction has been associated with the development of central pontinemyelinolysis, which may result in quadriplegia, cranial nerve abnormalities that manifest as pseudobulbar palsy, alteration in mental status, and subsequent death.
For patients with SIADH due to SCLC, treatment with chemotherapy should be initiated as soon as possible and is likely to result in improvement in the hyponatremia within a few weeks. • After an initial response to chemotherapy, SIADH may recur when the tumor relapses
Hypercalcemia • Hypercalcemia in association with malignancy may arise from a bony metastasis or, less commonly, from secretion by the tumor of a parathyroid hormone–related protein (PTHrP) or other bone-resorbing cytokine. • The most common cancers to cause hypercalcemia are those of the kidney, lung, breast, head, and neck and myeloma and lymphoma. • Squamous cell histology is the most common cell type associated with hypercalcemia, and generally patients have advanced disease (stage III or IV) and are unresectable.
Symptoms of hypercalcemia include anorexia, nausea, vomiting, constipation, lethargy, polyuria, polydipsiaand dehydration. Confusion and coma are late manifestations, as are renal failure and nephrocalcinosis. • Cardiovascular effects include shortened QT interval, broad T wave, heart block, ventricular arrhythmia, and asystole. Individual patients may manifest any combination of these signs and symptoms in various degrees. • Hypercalcemia of malignancy that is not caused by bony metastases results from accelerated bone resorption, decreased bone deposition, or increased renal tubular reabsorption of calcium.
Accelerated bone resorption is caused by activation of osteoclasts by cytokines or PTHrP in most cases. • Serum parathyroid hormone levels are usually normal or low, but an elevated level of PTHrP can be detected in the serum in approximately one half of these patients. Cytokines or PTHrP are secreted autonomously by the tumor. • Not only does PTHrP cause renal calcium reabsorption, but also it interferes with renal mechanisms for reabsorption of sodium and water, with resultant polyuria. • Polyuria and vomiting result in dehydration; decreases in glomerular filtration further aggravate the hypercalcemia.
Treatment: • Mild elevation of serum calcium may not require treatment, so the decision is based on the patient's symptoms. • For patients who have widely metastatic and incurable malignancy, it may be most appropriate to give supportive care only and not treat the hypercalcemia. The average life expectancy in this situation is 30 to 45 days, even with aggressive treatment.
Most patients who have a serum calcium of 12 to 13 mg/dL or higher are treated. • The four basic goals of treatment are to (1) correct dehydration; (2) increase renal excretion of calcium; (3) inhibit bone resorption; and (4) treat the underlying malignancy. • Because of the polyuria, patients with hypercalcemia are volume contracted. Initial treatment is with intravenous normal saline, using 3 to 6 L/24 hr as tolerated, with careful attention to volume status.
Zoledronate is given 4 mg intravenously over 15 minutes. • Adverse effects are generally mild and transient and include fever, hypophosphatemia, asymptomatic hypocalcemia and, occasionally, renal failure. • Calcitonin inhibits bone resorption, increases renal calcium excretion, and has a rapid onset of action, but the duration of action is short-lived.Given when the calcium is greater than 14 mg/dL or needs to be lowered urgently (onset of action is 4–6 hr)
The effects of calcitonin and bisphosphonates are additive. Tachyphylaxis may occur to calcitonin after 48 hours. • Thiazide diuretics are not used because they increase calcium reabsorption in the distal tubule. • Normal calcium levels are achieved within 4 to 10 days in 85% of patients and last a median of 30 to 40 days
Musculoskeletal Effectsclubbing of digits • May be a manifestation of lung cancer or other diseases. • Most commonly seen in adenocarcinoma of the lung and less frequently in other cell types. • Clubbing may involve the fingers and toes and consists of selective enlargement of the connective tissue in the terminal phalanges. • Physical findings include loss of the angle between the base of the nail bed and the cuticle, rounded nails and enlarged fingertips.
In digital clubbing proliferation of connective tissue beneath the nail matrix is observed. • Clubbing is an isolated finding and is usually asymptomatic. • Non-malignant causes of clubbing include pulmonary fibrosis, congenital heart disease, and bronchiectasis.
Hypertrophic pulmonary osteoarthropathy (HPO) • Is an uncommon process associated with lung cancer. • HPO is characterized by painful arthropathy that usually involves the ankles, knees, wrists, and elbows and is most often symmetrical. • The pain and arthropathy are caused by proliferative periostitis that involves the long bones but may also affect metacarpal, metatarsal, and phalangeal bones. Patients may have clubbing of fingers and toes in addition to the painful arthralgias.
The pathogenesis of HPO is uncertain, but it may arise from a humoral agent(VEGF/PDGF). • For patients who smoke and have a new onset of arthralgias, HPO must be considered • A radiograph of the long bones (i.e., tibia and fibula) usually shows characteristic periosteal new bone formation. An isotope bone scan typically demonstrates diffuse uptake by the long bones.
Large cell and adenocarcinoma are the most common histologic types associated with HPO. • The symptoms of HPO may resolve after tumour resection. • For inoperable patients, treatment is with nonsteroidal anti-inflammatory agents. Recently, case reports have observed resolution or marked improvement of symptoms with bisphosphonate treatment
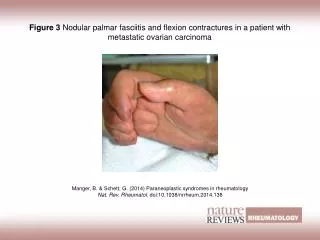
Dermatomyositis-polymyositis • Dermatomyositis and ploymyositis are associated with neoplasms in 40% of all cases. • Besides ovarian cancer SCLC is the most frequent type of cancer. • Dermatomyositis is characterized by infarcts, perifascicular atrophy , endothelial cell swelling and necrosis, vessel wall membrane attack complex deposition and myocyte-specific MHC-1 upregulation in the muscle. • Histopathological findings include hyperkeratosis , epidermal basal cell vacuolar degeneration and apoptosis,increased dermal mucin deposition cell poor interface dermatitis.
Myositis is charcterized by muscle weakness and muscle pain. • Typically proximal muscles are involved. • Myositis-specific autoantigens are expressed at high levels in regenerating cell in myositic muscles and cancer cells. This may provide a link between cancer and paraneoplasticmyositic syndrome.
Hematologic/vascular Effects • Anemia frequently occurs in patients who have lung cancer and may be caused by iron deficiency, chronic disease, or bone marrow infiltration. • Eosinophilia is more commonly associated with Hodgkin's disease but may occur in patients who have lung cancer. • Production of various cytokines by neoplastic cells may result in eosinophilia, leukocytosis, or thrombocytosis, of which thrombocytosis is by far the most common.
The association of deep venous thrombosis and malignancy was described by Trousseau over a century ago, and lung cancer is the most common malignancy associated with Trousseau's syndrome • Thromboembolism in the patient who has malignancy is often refractory to warfarin treatment. • Treatment with low-molecular-weight heparin (LMWH) on a chronic basis may be effective
. • In a randomized trial, patients with cancer and deep vein thrombosis, pulmonary embolism, or both were randomized to receive LMWH (dalteparin) subcutaneously once daily or oral warfarin daily for 6 months. • At 6 months, the probability of recurrent thromboembolism was 9% with dalteparin treatment and 17% with warfarin, a difference that was highly significant. • The risks of major bleeding or any bleeding were not different in the two groups. • The other advantage of LMWH is that it is unnecessary to monitor the anticoagulant effect, except in some patients with renal insufficiency. • A recent Cochrane analysis concluded that, for long-term treatment in patients with cancer, LMWH reduced venous thromboembolism events, but not death, as compared with vitamin K antagonists. There was no significant difference in the risk of bleeding.
Granulocytosis • Granulocytosis with absolute cell count of 10,000 to 25,000 occurs in 20% of patients of non-small cell lung cancer. • The specific ectopic harmone responsible for paraneoplasticgranulocytosis has not been characterized, although some non-small celtumours may produce various cytokines like IL-6, G-CSF or GM-CSF. • Bone marrow biopsy is usually normal. • Diagnosis is made on exclusion, granulocytosis per se does not produce any symptom in these patients.
Thrombocytosis • It is common phenomena observed in 40% patients of both small cell and non small cell carcinomas. • Exact mechanism of thrombocytosis is not known, it is most likely linked to megakaryocyte cytokine i.e. IL-6. • It is asymptomatic , diagnosed if bone marrow biopsy is normal and platelet count exceeds 500,000/mm2.
Acromegaly • Carcinoidtumour is the most common cause of acromegaly associated with lung cancer. • SCLC can also produce acromegaly. • Its due to the release of GHRH & rarely by GH. • Pts develop thick leathery skin, prominent skin folds, hypertrophy of face & extremities, diabetes & hypertension.
Increased levels of GHRH & IGF-1 in presence of lung tumour establishes diagnosis. • Respond to surgical resection as well as radiotherapy. • Pts ineligible for resection/irradiation should receive octreotide, which inhibits GHRH secretion form the tumour & decreases GH & IGF-1 levels in serum.
Neurologic Effects • The paraneoplastic neurologic syndromes associated with lung cancer, mostly small cell type, are quite variable. They include LEMS, subacute sensory neuropathy, encephalomyelopathy, cerebellar degeneration, autonomic neuropathy, retinal degeneration, and opsoclonus. • The frequency of any of these neurologic syndromes in SCLC is approximately 5%, and neurologic symptoms may precede the diagnosis by months to years.
Careful radiographic evaluation of the lungs and mediastinum is indicated in a smoker who has a suspected paraneoplastic neurologic syndrome. • In this setting, even subtle abnormalities of the mediastinum require a biopsy. A PET scan may help identify an occult lesion and facilitate biopsy confirmation of the diagnosis.