Download
1 / 51
730 likes | 2.89k Views
Diseases of the Larynx. Khalid H. Al-Sebeih, MD, FRCSC, ABO Assistant Professor, Department of Surgery Faculty of Medicine, Kuwait University. Department of Otolaryngology, Sabah Hospital. Anatomy. Clinical subdivision Supraglottis:

E N D
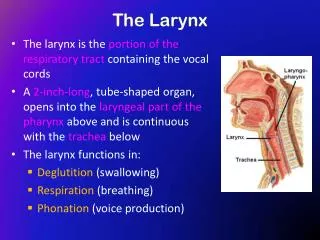
Diseases of the Larynx Khalid H. Al-Sebeih, MD, FRCSC, ABO Assistant Professor, Department of Surgery Faculty of Medicine, Kuwait University. Department of Otolaryngology, Sabah Hospital
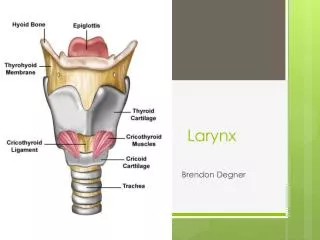
Anatomy • Clinical subdivision • Supraglottis: • from epiglottic tip to floor of laryngeal ventricle ( SE & RE junction). • Glottis: • ant. commissure, TVC, post commissure • Subglottis: • SE & RE junction at the inf. surface of TVC to inferior edge of cricoid (5 mm below TVC)
Anatomy • Laryngeal spaces • Paraglottic space: thyroid lamina, quadrangular memb, conus elasticus • Pre-epiglottic space: vallecular mucosa, thyroid cart., thyrohyoid memb., epiglottis
Diseases of the Larynx • Inflammatory • Infectious • Granulomatous • Mucosal • Congenital • Neoplastic
3 years old boy • Presented with: • Stridor: 1 day • Cough, barking • Fever • Drooling??
Inflammatory • Acute laryngotracheitis • viral infection, affects children < 5 years. • lasts 3-7 days, seasonal, in autumn & winter. • parainfluenza 1, parainfluenza 3, influenza A, rhinovirus. • febrile URTI, followed by classic barky or croupy cough (nonproductive and at night. • self-limited, rarely edema & upper A/W obstruction. • Dx: history + neck X-ray classic “steeple sign”. • Tx: humidification & hydration. If symptoms worsen racemic epinephrine & corticosteroids
Acute epiglottitis • Haemophilus influenzae type B • Children between 2 - 4 years, winter and spring. • Rapid presentation over 2-6 hrs: fever, sore throat, muffled voice, inspiratory stridor. Sitting upright, ill-appearing, &drooling, • Examination of the epiglottis may precipitate laryngospasm not recommended. • Lateral X-ray classic “thumb” sign. • Tx: operating room immediately to establish the diagnosis and secure an airway
Acute epiglottitis • Treatment: • Secure a safe airway (O-T tube, bronchoscope, trach) • Antimicrobial (C/S) ampic & chloramphenicol or 2nd & 3rd generation cephalosporin. • Supportive care. Extubation usually possible after 48 to 72 hours
Croup Vs Epiglottitis Characteristics of Laryngotracheitis and Epiglottitis Feature Laryngotracheitis Epiglottitis Age <3 years >3 years Onset Gradual (days) Acute (hours) Cough Barky Normal Posture Supine Sitting Drooling No Yes Radiograph Steeple sign, narrowed subglottis Thumb sign, enlarged epiglottis,dilated hypopharynx Cause Viral Bacterial Treatment Supportive (croup tent) Airway management (intubation or tracheotomy), antibiotics
40 years old lady • Globus pharyngeus • Dryness of throat • Frequent throat clearing • Nocturnal aspiration • Heart burn
Gastroesophageal reflux disease - GERD • Most common cause of laryngitis. • Acute & chronic • GERD stenosis, recurrent spasm, C-A fixation, dysphagia, globus pharyngeus, & laryngeal CA. • Sx: • GI: regurgitation, heart burn. • Larynx: hoarseness, globus pharyngeus, ch. Throat clearing, cough, dysphagia.
Gastroesophageal reflux disease - GERD • Examination: • Grade I : Normal or Mild Edema & Erythema • Grade II : Erythema / Edema of posterior glottis. • Grade III : Pachydermia of posterior glottis. • Grade IV : Contact ulcer granuloma
GERD • Dx: • Hx • Examination • 24-hour double probe PH monitoring. • Ba-swallow. • Gastroscope
GERD • Treatment: • Dietary and Lifestyle modifications. • Antacids. • Systemic H2-blockers. • Prokinetic agents. • Mucosal cytoprotectants. • Proton pump inhibitors; Omebrazole
Other inflammatory disease Granulomatous Conditions That May Affect the Larynx Disease Laryngeal Involvement Tuberculosis Posterior one-third of larynx involved Syphilis Painless ulcers; positive syphilis serology Leprosy Supraglottic involvement Histoplasmosis Anterior larynx involved Blastomycosis Painless ulcers; microabscesses Actinomycosis Draining sinuses; sulfur granules Rhinoscleroma Catarrhal stage, Mikulicz’s cells Sarcoidosis Supraglottic swelling, nodules, granulomas Wegener’s Subglottic involvement; necrotizing vasculitis; pulmonary or granulomatosis renal involvement
33 years old lady • Teacher • Hoarseness of voice • Cough mild • Disappearance of voice sometimes • No h/o URTI
Benign mucosal disorder • Vocal nodule • Fluid accumulation in the submucosa from acute abuse or overuse mucosal swelling (sometimes called "early nodules"): reversible. • Long-term voice abuse hyalinization of Reinke's potential space, irreversible. • Tx: • Medical: hydration, lubrication, GERD. • Voice therapy • Surgery: >3months, fibrosis, symptomatic.
Saccular Disorders • small out-pouching at anterior end of laryngeal ventricle saccule. • Contains mucous glands & empties through an orifice located in the anterior part of the ventricle. • saccular disorders: laryngocele or saccular cyst.
Laryngocele • Laryngocele saccule is filled only • classifications: internal, external, and combined. • etiology • transglottic pressure, e.g. in trumpet players • laryngeal carcinoma partial obstruction • Congenital • Sx: hoarseness, neck swelling, stridor, dysphagia, sore throat, and cough. • Tx: • internal endoscopic marsupialization • External or combined external approach
Saccular cyst • Saccular cysts: Anterior & Lateral • Cyst filled with glandular secretions, 2nd to orifice obstruction. • Sx: hoarseness , dyspnea, dysphagia, pain, and a neck mass • Tx: same to laryngocele
2 weeks old girl • Inspiratory stridor • No cyanosis • Normal cry • No chest infection • Aspiration with feeding
Laryngomalacia • Abnormal flaccidity of the laryngeal tissues inward collapse. • Resolve spontaneously (6-18 months). • Sx: inspiratory stridor, intermittent upper a/w obstruction, normal cry, normal general health and development • Usually begins in the first few days or weeks.
Laryngomalacia • Dx: endoscopic exam. • Tall, tubular, epiglotttis • Large cuniform cartilage. • Short A-E folds • Inward collapse • Tx • Conservative:posturing, +/- steroids • Surgical: trach, intubation, supraglottoplasty
Vocal cord paralysis (cong.) • 2nd common cause of congenital upper a/w obstruction. (10%) • Unilateral VC paralysis > bilateral • Causes: idiopathic, surgical trauma, neurological abnormalities (e.g. meningomyelocele, bulbar palsy, Arnold-Chiary malformation. • Sx: weak cry, aspiration, stridor. • Tx: • Surgical: trach, transverse cordotomy, arytenoidectomy.
Subglottic stenosis • Membranous and cartilaginous types. • Membranous: fibrous soft-tissue thickening of the subglottic area • Cartilaginous: thickening or deformity of the cricoid cartilage shelf-like plate • Grading of laryngeal stenosis • Grade I Less than 70% • Grade II 70%-90% • Grade III More than 90%; • Grade IV Complete obstruction
Subglottic stenosis • Tx: • Endoscopic: membranous stenosis • Surgery: cartilaginous stenosis • Ant cricoid split • Ant. & post cricoid division +/- augmentation
Laryngeal Hemangioma • Infants 50% associated cutaneous hemangiomas. • Sx: stridor or "pseudocroup," within the first 6 months of life. • Dx: direct laryngoscopy • Tx:low-dose XRT, tracheotomy + observation, cryotherapy, sclerotherapy, CO2 laser, steroid therapy (systemic or intralesional) & interferone -2a.
55 years old gentleman • Hoarseness of voce • Right otalgia • Mild dyspyagia • Smoker • Alcohol drinker
Laryngeal Papillomatosis • The most common benign neoplasms of the larynx (84% of benign tumors). • 2nd mucosal infection by a papovavirus. • Juvenile form: • diffuse & extremely aggressive hoarseness and stridor. • Resistant to treatment frequent laryngoscopies. • Adult-onset form • solitary or more localized, less aggressive • TX:CO2 laser, cryotherapy, XRT, interferon
Sqaumous cell Carcinoma • Most common laryngeal Ca (>90%). • Male:female = 6:1. • Etiology: • Tobacco: (related to number of cig.) • Alcohol: (x 2.2) • XRT, asbestose, wood dust, mustard gas. • GERD • HPV
Sqaumous cell Carcinoma • Glottic SCCA most common (60%) > supraglottic SCCA (30%) > subglottic SCCA (<10%). • Sx: hoarseness, throat pain, cough, hemoptysis, referred otalgia, dysphagia. • Dx: • Flexible laryngoscope, D.L. & biops. • CT +/- MRI
Sqaumous CCA (TNM staging) T: primary tumor Tx Cannot be staged T0 No evidence of tumor Tis Carcinoma in situ Supraglottis T1 Tumor confined to one subsite of larynx; normal mobility (i.e., ventricular bands; arytenoids; epiglottis) T2 Involving more than one subsite (supraglottis or glottis; normal mobility) T3 Linked to larynx with fixation or extension to involve postcricoid, medial pyriform, or preepiglottic space T4 Tumor invasion of cartilage or tissue beyond larynx Glottis T1 Tumor limited to vocal cords, normal mobility T1a one cord T1b both cords T2 Extension to supraglottis and/or subglottis; may be impaired cord mobility T3 Limited to larynx with cord fixation T4 Extension beyond larynx or into cartilage Subglottis T1 Tumor limited to subglottis T2 Extension to vocal cord; mobility may be impaired T3 Limited to larynx with cord fixation T4 Extension beyond larynx or into cartilage
Sqaumous CCA (TNM staging) N: regional nodes Nx Cannot be assessed N0 No regional metastasis N1 Single positive ipsilateral node, less than 3 cm N2 Nodes less than 6 cm N2a Single ipsilateral node 3-6 cm N2b Many ipsilateral nodes less than 6 cm N2c Bilateral and contralateral node less than 6 cm N3 Node(s) greater than 6 cm M: distant metastasis Mx Cannot be assessed M0 No distant metastasis M1 Distant metastasis Stage grouping 0 Tis N0 M0 I T1 N0 M0 II T2 N0 M0 III T3 N0 M0 T1-3 N0 M0 IV T4 or N2-3 or M1
Sqaumous CCA • Tx: • Glotiic: • T1, T2: • XRT or Partial resection (cordectomy, partial laryngectomy) • good prognosis (>90% 5 yrs survival) • T3: • XRT for organ preservation & Surgery for salvage • Surgery (total laryngectomy) + post op XRT • T4: • Combined Surgery (total laryngectomy & ND) + XRT
Sqaumous CCA • Tx: • Supraglotiic & subglottic • T1, T2: • XRT or Partial resection (cordectomy, partial laryngectomy) • good prognosis (>90% 5 yrs survival) • T3, T4: • Combined Surgery (total laryngectomy & ND) + XRT • Prognosis: • Stage dependent • T1,T2: >80% 5 yrs survival • T3: 50-60% • T4: < 40% • N+: reduce prognosis by half