Download
1 / 98
1.01k likes | 1.32k Views
PNEUMONIA. ALOK SINHA Department of Medicine Manipal College of Medical Sciences Pokhara , Nepal. Acute respiratory illness of varied aetiology associated with recently developed radiological opacities which can be- Segmental Lobar Multilobular.

E N D
PNEUMONIA ALOK SINHA Department of Medicine Manipal College of Medical Sciences Pokhara, Nepal
Acute respiratory illness of varied aetiology associated with recently developed radiological opacities which can be- • Segmental • Lobar • Multilobular
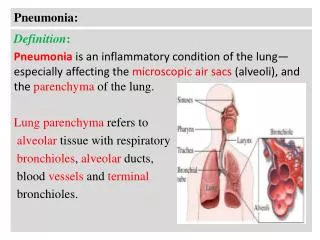
Pneumonia is parenchyma/alveolar inflammation of lungs and abnormal alveolar filling with fluid. . Pneumonia is parenchyma/alveolar inflammation of lungs and abnormal alveolar filling with fluid. Type of V/Q mismatch ??
Classification Anatomic or Pathologic • Lobar (or segmental) pneumonia • infection of a single lobe often due to Streptococcus pneumoniae (some times segmental) • Multilobar pneumonia(Broncho pneumonia) • involves more than one lobe, and it often causes a more severe illness • Interstitialpneumonia • involves the areas in between the alveoli
Atypical pneumonia • caused by agents such as • Mycoplasma • Legionella • Chlamydia • Coxiella burnetii • clinical features of these pneumonias can differ from pneumococcal disease • Account for 20% cases of pneumonia
Combined clinical classification • Community-acquired pneumonia (CAP) • Hospital-acquired pneumonia(nosocomial)
Community-acquired pneumonia (CAP) is an infection of the alveoli, distal airways, and interstitium of the lungs that occurs outside the hospital setting • Characterized clinically by: • Fever • Chills • Cough • Pleuritic chest pain • Sputum production • At least one opacity on chest radiography
Epidemiology • Incidence: • 800–1500 cases per 100,000 persons annually • ~20% require hospitalization • Age • Incidence highest at extremes of age • Sex • Rate higher among men than among women • Seasonality • More common during the winter/spring months
Low mortality rate in adults < 1% at home • Is high in children-20% of childhood deaths • Most cases in previously healthy persons • Impairment of local defense mechanism predisposes to Pneumonia
Risk Factors • Independent risk factors for CAP include: • Alcoholism [relative risk (RR) 9] • Cigarette smoking • Asthma (RR 4.2) • Immunosuppression (RR 1.9) • Corticosteroid therapy • Multiple myeloma • Spleenectomy • H.I.V. • Age >70 years (RR 1.5 vs. 60–69 years) • URTIs • Pre existing lung disease
Common • S. pneumoniae - most common cause of community-acquired bacterial pneumonia • H. influenzae • K. pneumoniae Uncommon • S. aureus • S. pyogenes • P. aeruginosa • N. meningitidis Rare • Y. pestis • B. pseudomallei • Acinetobacter calcoaceticus
S pneumoniae -common cause of bacterial pneumonia. Colonizes upper respiratory tract and can cause the following: • a) disseminated invasive infections, including bacteremia and meningitis • b) pneumonia and other lower respiratory tract infections • c) upper respiratory tract infections, including otitis media and sinusitis • H influenzae often is associated with debilitating conditions such as asthma, COPD, smoking, and a compromised immunesystem
K pneumoniae -severe necrotizing lobar pneumonia in patients with chronic alcoholism,diabetes, or COPD • S aureus in intravenous drug users. in hospitalized patients, with prosthetic devices, people with a recent influenza virus infection, and in individuals with cystic fibrosis • L pneumophila infections occur either sporadically or as local outbreaks from contaminted air conditioners
Microaspiration of oropharyngeal secretions colonized with pathogenic microorganisms • S. pneumoniae • H. influenzae is most common route – Community acquired pneumonia
Gross aspiration • Central nervous system disorders that affect swallowing (e.g., stroke, seizures) • Impaired consciousness (e.g., in alcoholism, IV drug use) • Anesthesia or intubation • Pathogens include anaerobic organisms and gram-negative bacilli -Common in Hospital acquired pneumonia
Other less important • Aerosolization • Hematogenous spread • Contiguous spread from another site
Clinical Features Clinical features = Symptoms + Signs
Stages of pneumonia • Consolidation • Red hepatization • Gray hepatization • resolution
History • Most typical signs/symptoms – depends upon the stage of disease • Fever • Cough • Nonproductive initially • productive of purulent sputum latter stages • Pleuritic chest pain • Occasionally referred to the shoulder or anterior abdominal wall & associated with upper abdominal tenderness • Chills and/or rigors • Dyspnea
Frequent signs/symptoms • Headache • Nausea • Vomiting • Diarrhoea • Fatigue • Arthralgia/myalgia • new-onset or worsening confusion (in elderly patients) • herpes labialis
Character of sputum produced may suggest a particular pathogen • Pneumococcal pneumonia bloody or rust-colored • Pseudomonas, Haemophilus- green sputum • Anaerobic infections- foul-smelling and bad-tasting • Klebsiella or pneumococcal species- Currant-jelly endobronchial plug of blood, sputum, mucus & debris
Fever • Tachypnea (Accessory muscles – active) • Tachycardia • Cyanosis Chest examination • Chest expansion – restricted • Percussion - impaired • Increased tactile and vocal fremitus • BRONCHIAL BREATH SOUNDS present • Egophony & Whispering pectoriloquy • Crackles • Pleural friction rub
Differential Diagnosis • Infections • Lung abscess • Bronchitis • Noninfectious illnesses • Pulmonary embolism • Pulmonary hemorrhage • Pulmonary edema • Pulmonary fibrosis/scarring • Inflammatory disorders • Sarcoidosis • Wegener’s granulomatosis • Other rheumatologic/vasculitic diseases • Lung cancer • Hypersensitivity pneumonitis • Bronchiolitis obliterans organizing pneumon (BOOP)
Assess pneumonia severity • Pay attention to vital signs, including oxygen saturation • Always count the respiratory rate yourself for 1 min • The single most useful clinical sign of severity is a respiratory rate of >30/min in a person without underlying lung disease
CURB65SCORE 7 mmol/l or 42mg/dl (Blood Urea Nitrogen>19)
The main objectives of investigating patients with a clinically based diagnosis of pneumonia are: • to obtain radiological confirmation of diagnosis • exclude other conditions that mimic pneumonia • to obtain a microbiological diagnosis • to assess the severity of pneumonia • to identify the development of complications
INVESTIGATIONS Depends on the severity of diseases CURB65 score 0 can be managed empirically Score 1-2: a. Sputum examination with gram & ZN stain b. Blood culture c. Serology-Acute & convalescent titers Score > 2: All the bove + a. Tracheal aspirate b. B.A.L. c. Serology-Legionella antigen in urine Pneumococcal in sputum & blood d. Throat swab and pleural fluid if present
Laboratory Tests • Nonspecific studies • Complete blood count • Serum electrolyte and glucose measurements • Blood urea nitrogen (BUN) and creatinine measurements • Arterial blood gas & Pulse oximetry
Sputum stains and culture • Gram’s stain • Useful in screening a sputum sample for suitability for culture and in making a presumptive etiologic diagnosis • A sputum sample with • >25 white blood cells (WBCs) • <10 squamous epithelial cells per low-power field is suitable for culture • Most common: presence of gram positive diplococci – S. Pneumonae
Other sputum stains that may be helpful in some patients • Stains for • Acid-fast bacilli • Pneumocystis • Fungi • Cytology (malignancy) • Rapid antigen testing for viral pathogens (e.g.Influenza)
Sputum culture • Results should always be correlated with those of Gram staining (of sputum) • If an organism is isolated from sputum and is morphologic correlate is not seen on Gram staining, the isolate may be colonizing the upper airway
Certain microorganisms, if isolated from sputum, should always be considered pathogens. These include: • M. tuberculosis • Legionella spp. • Blastomyces dermatitidis • Histoplasma capsulatum • Coccidioides immitis (Only about one-third of elderly patients admitted with CAP produce sputum suitable for culture)
Blood culture Indications: • Hyperthermia (body temperature >38.5°C) • Hypothermia (body temperature <36°C) • Homeless • Alcohol abuse
All patients admitted to the hospital for CAP should have 2 sets of blood cultures done before initiation of antibiotic therapy (positivity rate: 6–20%) • Most common isolates • S. pneumoniae (~60%) • S. aureus • Escherichia coli
Detection of antigens of pulmonary pathogens in urine • S. pneumoniae • The antigen detected for up to 1 month after the onset of pneumonia • results can be available in 15 min • L. pneumophila • when Legionnaires’ disease is strongly suspected • Rapidly progressive pneumonia • Urine antigen test most frequently used diagnostic method for Legionnaires’ disease
Serology • Detection of IgM antibody • 4-fold rise in titre of antibody to a particular agent between acute & convalescent phase indicates is the cause of CAP • Useful for epidemiological study
Chest x-ray • Diagnostic test of choice for pneumonia • May show • Lobar or segmental consolidation • Bronchopneumonic pattern • Interstitial infiltrates • Cavitation • Associated pleural fluid, etc
The common patterns in pneumonia are- segmental or lobar pneumonia – • Strep. pneumoniae • Mycoplasma. pneumoniae • Legionella. pneumophila • Staph. aureus • C pneumoniae • Mycobacterium tuberculosis
Left upper lobe pneumonia Air bronchogram
Left upper lobe consolidation Same patient as in previous one