Download
1 / 43
450 likes | 598 Views
Characteristics. 1) SLD, 2) SLI 3 ) MR 4 ) ED SLD, SLI, MR, and ED accounts for 88% of all students with disabilities. Typical language development Structured, shared, rule-governed, symbolic system for communicating

E N D
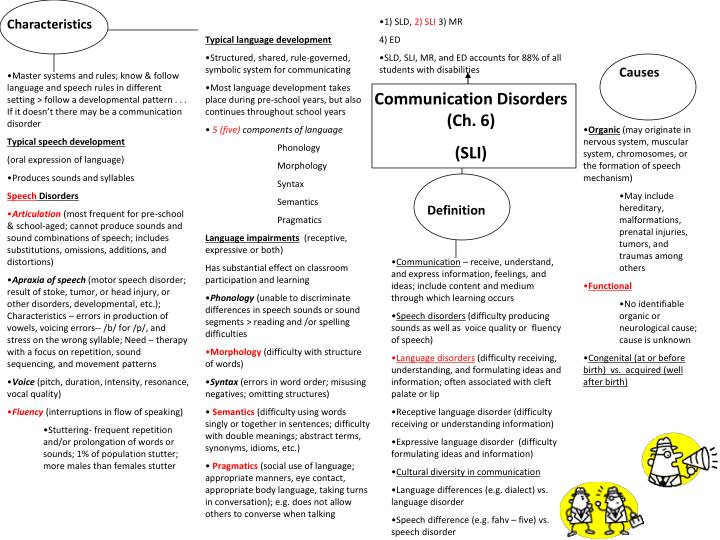
Characteristics • 1) SLD, 2) SLI 3) MR • 4) ED • SLD, SLI, MR, and ED accounts for 88% of all students with disabilities • Typical language development • Structured, shared, rule-governed, symbolic system for communicating • Most language development takes place during pre-school years, but also continues throughout school years • 5 (five) components of language • Phonology • Morphology • Syntax • Semantics • Pragmatics • Language impairments (receptive, expressive or both) • Has substantial effect on classroom participation and learning • Phonology (unable to discriminate differences in speech sounds or sound segments > reading and /or spelling difficulties • Morphology (difficulty with structure of words) • Syntax (errors in word order; misusing negatives; omitting structures) • Semantics (difficulty using words singly or together in sentences; difficulty with double meanings; abstract terms, synonyms, idioms, etc.) • Pragmatics(social use of language; appropriate manners, eye contact, appropriate body language, taking turns in conversation); e.g. does not allow others to converse when talking Causes • Master systems and rules; know & follow language and speech rules in different setting > follow a developmental pattern . . . If it doesn’t there may be a communication disorder • Typical speech development • (oral expression of language) • Produces sounds and syllables • SpeechDisorders • Articulation (most frequent for pre-school & school-aged; cannot produce sounds and sound combinations of speech; includes substitutions, omissions, additions, and distortions) • Apraxia of speech (motor speech disorder; result of stoke, tumor, or head injury, or other disorders, developmental, etc.); Characteristics – errors in production of vowels, voicing errors-- /b/ for /p/, and stress on the wrong syllable; Need – therapy with a focus on repetition, sound sequencing, and movement patterns • Voice (pitch, duration, intensity, resonance, vocal quality) • Fluency (interruptions in flow of speaking) • Stuttering- frequent repetition and/or prolongation of words or sounds; 1% of population stutter; more males than females stutter Communication Disorders (Ch. 6) (SLI) • Organic (may originate in nervous system, muscular system, chromosomes, or the formation of speech mechanism) • May include hereditary, malformations, prenatal injuries, tumors, and traumas among others • Functional • No identifiable organic or neurological cause; cause is unknown • Congenital (at or before birth) vs. acquired (well after birth) Definition • Communication – receive, understand, and express information, feelings, and ideas; include content and medium through which learning occurs • Speech disorders (difficulty producing sounds as well as voice quality or fluency of speech) • Language disorders(difficulty receiving, understanding, and formulating ideas and information; often associated with cleft palate or lip • Receptive language disorder (difficulty receiving or understanding information) • Expressive language disorder (difficulty formulating ideas and information) • Cultural diversity in communication • Language differences (e.g. dialect) vs. language disorder • Speech difference (e.g. fahv – five) vs. speech disorder
Knowledge of the Psychology of Reading and Reading Development • Learning to read is an acquired skill; it is NOT natural or easy • Children who learn to read well are sensitive to linguistic structure • Recognize redundant patterns • Connect letter patterns with sounds, syllables, word parts • Effective teaching of reading should be presented in an order in which children can learn (systematic and explicit) • Reading calls for deep linguistic processing • Language knowledge and proficiency differentiate good and poor readers • Instruction that benefits those learning to read: • Develops awareness of sounds, syllables, word parts, relationships among word meanings, and the structures of written text • Language skills that distinguish good vs. poor readers • Phonological system • Awareness of linguistic units that lie within a word (consonants, vowels, syllables, grammatical endings, word parts, and the spelling units); fluency in recognition and recall of letters and spelling patterns that make up words
Language Structure(Linguistics: The scientific study of language) • Reading is a language based skill • Teaching children to read requires teaching them language at a higher and conscious level • Language, an immutable aspect of literacy • Components of language • Phonology • Morphology • Syntax • Semantics • Pragmatics
Phonology • The smallest linguistic unit of sound that can change meaning in a word • 26 letters with which represent approximately 44 phonemes of English • 5 vowel letters to represent 15 vowel sounds • Knowledge of phonemes and their role in language and reading is essential for teachers • How do children learn phonemes? Being exposed to them, by hearing others speak, by storing information about the qualities that make up each sound • Typically developing children are able to produce speech sounds adequately by age 4 and require additional time for complete mastery (age 7) • Phonological awareness abilities have been identified a critical to the development of early reading • Phonological skills are relevant to early decoding • Early reading ability is strongly connected to phonological knowledge as is the later development of spelling
Morphology • Study of word formation • Morpheme: smallest units of meaning in language • Endowed with meaning • Morphological awareness has been shown to be a strong indicator of reading comprehension • Morphological knowledge adds to the skills required for spelling and comprehension • Later reading development , fluency and comprehension, have their roots in morphology and syntax while relying on efficient phonological processing • Words are made up of one or more morphemes • E.g. smile, book, cute> how many morphemes? • Types of morphemes • Unbound (morpheme that can stand alone) • Have lexical (word) meaning of their own • Bound (must be attached to other morphemes) • Affixes (prefixes and suffixes) • -un, -ing, -s, -est • Either inflectional • or derivational • Inflectional (modify tense, possession, or number) • Derivational (change one part of speech to another)
Syntax (grammar) • System of rules that directs the comprehension and production of sentences • Specifies the order of words and organization of words within a variety of sentence types • Allows users to combine words into meaningful sentences and to alter the form of a sentence • Significant to fluency and comprehension in later reading development • Knowledge of syntactic structure helps an individual to predict the likelihood of either an adjective or noun or both coming next • Early syntactic delay were predictive of subsequent reading disability
Semantics • Meaning component of language • Concerned with the meanings of words and the relationship between and among words as they are used to represent knowledge of the world • Children with reading deficits have been shown to have difficulties in vocabulary, word categorization, and word retrieval • Other aspects of semantics • synonyms • Antonyms • Similes • metaphors
Pragmatics • Social uses of language
Characteristics • 1) SLD, 2) SLI 3) MR • 4) ED • SLD, SLI, MR, and ED accounts for 88% of all students with disabilities • Typical language development • Structured, shared, rule-governed, symbolic system for communicating • Most language development takes place during pre-school years, but also continues throughout school years • 5 (five) components of language • Phonology • Morphology • Syntax • Semantics • Pragmatics • Language impairments (receptive, expressive or both) • Has substantial effect on classroom participation and learning • Phonology (unable to discriminate differences in speech sounds or sound segments > reading and /or spelling difficulties • Morphology (difficulty with structure of words) • Syntax (errors in word order; misusing negatives; omitting structures) • Semantics (difficulty using words singly or together in sentences; difficulty with double meanings; abstract terms, synonyms, idioms, etc.) • Pragmatics(social use of language; appropriate manners, eye contact, appropriate body language, taking turns in conversation); e.g. does not allow others to converse when talking Causes • Master systems and rules; know & follow language and speech rules in different setting > follow a developmental pattern . . . If it doesn’t there may be a communication disorder • Typical speech development • (oral expression of language) • Produces sounds and syllables • SpeechDisorders • Articulation (most frequent for pre-school & school-aged; cannot produce sounds and sound combinations of speech; includes substitutions, omissions, additions, and distortions) • Apraxia of speech (motor speech disorder; result of stoke, tumor, or head injury, or other disorders, developmental, etc.); Characteristics – errors in production of vowels, voicing errors-- /b/ for /p/, and stress on the wrong syllable; Need – therapy with a focus on repetition, sound sequencing, and movement patterns • Voice (pitch, duration, intensity, resonance, vocal quality) • Fluency (interruptions in flow of speaking) • Stuttering- frequent repetition and/or prolongation of words or sounds; 1% of population stutter; more males than females stutter Communication Disorders (Ch. 6) (SLI) • Organic (may originate in nervous system, muscular system, chromosomes, or the formation of speech mechanism) • May include hereditary, malformations, prenatal injuries, tumors, and traumas among others • Functional • No identifiable organic or neurological cause; cause is unknown • Congenital (at or before birth) vs. acquired (well after birth) Definition • Communication – receive, understand, and express information, feelings, and ideas; include content and medium through which learning occurs • Speech disorders (difficulty producing sounds as well as voice quality or fluency of speech) • Language disorders(difficulty receiving, understanding, and formulating ideas and information; often associated with cleft palate or lip • Receptive language disorder (difficulty receiving or understanding information) • Expressive language disorder (difficulty formulating ideas and information) • Cultural diversity in communication • Language differences (e.g. dialect) vs. language disorder • Speech difference (e.g. fahv – five) vs. speech disorder
Communication/ Language Disorders continued . . . Nondiscriminatory evaluation Progress in the General Curriculum • Observation • Medical personnel observe delays in communication developmental milestones • Teachers and parents observe that the child has difficulty • Screening (vision and hearing; classroom work products) • Pre-referral (typically not used); but if it is the general education teacher implements suggestions such as modeling speech sounds, asking the child open-ended questions) • Referral (child performs poorly in spite of interventions) • Non Discriminatory Evaluation • Assessment measures • IQ • Achievement tests • Speech and language tests • Oral-muscular functioning • Adaptive behavior scales • Curriculum-based assessment • Direct observation Collaboration • All professionals involved • May lighten everyone’s workload • Partnership with Speech Language Pathologist • UDL • Adapt instruction • Asking varied types of questions • Help students expand their utterances by adding more information or creating a more complete sentence • Providing statements that explain a student’s nonverbal behaviors • Respond positively to students’ utterances • Opportunity to practice public verbalizations • Some students may need to use AAC systems to express thoughts and ideas • Graphic organizer modification • Augment Instruction • Repetition of the curriculum • Visual supports (e.g. graphic organizers) • Direct instruction in social skills Prevalence • Inclusion • Majority spend day in general education • 18.7 % of students with disabilities; • 2ndmost prevalent disability category Assistive Technology Dragon Naturally Speaking- voice recognition software http://www.dragontalk.com/NATURAL.htm
Partnership with Speech Language Pathologist Teachers and SLP’s working with each other to support access to the general curriculum for students receiving special education and related services Consultation (SLP works with general educator to adapt materials) Provide more visual representations of content Supportive Teaching (SLP and general educator meet to plan extra supports a student will need in an upcoming unit) SLP can pre-teach vocabulary May meet with student after lesson to clarify and information he did not understand Complementary Teaching SLP takes notes for a student while the teacher teaches Provides/prepares study guides Teach small groups within the class that need more adaptation Teach organizational skills to whole class Universal Design – Modifications to how content is presented & how students demonstrate their knowledge Vary the way in which you communicate with students (how content is presented) Audio formats Text formats OR Talking books Visual representations with verbal information Graphic organizers Controlled vocabulary Demonstrate knowledge (how students demonstrate their knowledge) Ppt presentation, give a demonstration with visual supports, perform a skit or solo Instructional strategies Provide visual and verbal models Provide positive feedback Provide lots of opportunities for practice Graphic organizers (helps them learn and remember information) Supports SLI ASHA, 2003 (American Speech-Language-Hearing Association)
Facilitative Language Strategies • Focused contrast: by adult to show the child the difference between his or speech and the adult’s speech • Modeling: used to help a child learn a language or speech structure he or she doesn’t yet use • Event casts: provides an ongoing description of an activity while it is happening • Open questions: questions that have a variety of possible answers • Expansions: the adult repeats the child’s utterance, filling in the missing components • Graphic Organizers
Augmentative Communication • Check out these sources! • http://www.augcominc.com/whatsnew/ncs5.html • a dedicated speech-generating device • A few examples: • SpeechEasy(http://www.speecheasy.com/howitworks.php?s_kwcid=speech%2520easy|5235943702&gclid=CNfnt8bUw6QCFZJl7AodESvpCw) • Screen readers (text to speech) • Speech recognition system (voice recognition; enter data through voice)
What do statistics tell us? • Those who exhibit challenging behaviors may be labeled as having a developmental disability, autism, mental retardation, emotional or behavior disorder, traumatic brain injury, or any other disability • Note: The focus is on students who have identified disabilities and who exhibit problem behaviors that interfere with their learning or the learning of others in the classroom • Many terms are used to describe emotional, behavioral, or mental disorders. Students with such conditions are categorized as having an emotional disturbance • In Fall 2006, 457,731 children and youth with emotional disturbance were provided special education and related services in public schools • Some studies report that ED is .7 % of the population where other studies report that students with emotional disturbance make up 14 to 22% of the school population. • Some characteristics and behaviors seen in children with emotional disturbances include: • Aggression/self-injurious behavior (acting out, fighting) • Hyperactivity (short attention span, impulsiveness) • Withdrawal • Learning difficulties • Immaturity • Anxiety disorder (e.g. phobia, panic disorder, eating disorder, post-traumatic stress disorder) • Mood disorder (e.g. depression, bipolar disorder) • Oppositional defiant disorder • Conduct disorder • Schizophrenia A Look at ED
Emotional Disturbance Definition Accompanied by one or more of the of the following characteristics over a long period of time and to a marked degree that adversely affects a child’s educational performance: • An inability to learn that cannot be explained by intellectual, sensory, or health factors • An inability to build or maintain satisfactory interpersonal relationships with peers and teachers • Inappropriate types of behavior or feelings under normal circumstances • A general pervasive mood of unhappiness or depression • A tendency to develop physical symptoms or fears associated with personal or school problems
Anxiety disorders • Includes separation anxiety disorder, generalized anxiety disorder, phobia, panic disorder, obsessive-compulsive disorder, and post-traumatic stress disorder • Students are: • Extremely conscientious with their school assignments • May have a tendency to avoid mistakes • Perfectionism affects them • Isolated from peers • Tend to avoid threatening social situations • The worry about school and the pressure to be perfect may result in physical symptoms such as tension, headaches, and stomachaches
Mood Disorder • Depression • Highest rates occur in adolescent females • Suicide is the 3rd leading cause of mortality among adolescents • Students have lower academic achievement and lower scores on intelligence tests during depressive episodes; experience fatigue and decreased interest in their depressive state • Bipolar disorder
Oppositional Defiant Disorder • Pattern of negative, hostile, disobedient, and defiant behaviors • Students may have loss of temper, arguments with adults. Refusal to cooperate with adult request, frequent rule-breaking, deliberate annoyance of others, blaming others for mistakes, misbehavior, low self-esteem, easily annoyed, expressed resentfulness and anger, and tendency for vindictiveness • Behaviors must have occurred for at least 6 months • Typically diagnosed during elementary years • Precursor of conduct disorders
Conduct Disorder • Persistent pattern of antisocial behavior that interferes with others’ rights or with schools’ and communities’ behavioral expectations • Severe and aggressive antisocial behavior ; often infringe on other students’ rights • Typically during the elementary school years that boys are identified as having conduct problems • Often students with conduct disorders also have attention deficit/hyperactivity disorder • Half of youth incarcerated have been identified as having an emotional or behavioral disorder • African-Americans are four times as likely as their European American peers to be incarcerated
Schizophrenia • Experience the following: • Delusions • an auditory hallucination • Disorganized expressive language • Disorganized or catatonic behavior • Loss of contact with behavior
Excludes social maladjustment (choose to break societal rules) • Inability or inappropriately: learning & interpersonal relationships • Inappropriate types of behaviors • unhappiness and/or depression • Physical symptoms or fears associated with school problems • Includes schizophrenia Characteristics Definition Causes • Emotional • Anxiety – excessive fear, worry and uneasiness (most common childhood disorder) ; includes eating disorders, post-traumatic stress disorder, phobias, panic disorders, obsessive-compulsive disorder • Mood - depression; bipolar disorder (depression and excited phases) • ODD (defiant behaviors, disobedience, hostile) • Conduct disorder (antisocial behavior) – includes aggression, physical harm, deceit, theft, serious rule violations • Schizophrenia (hallucinations, withdrawal, loss of contact with reality; occurs in late adolescence and early adulthood) • Behavioral • Externalizing (aggressive, acting out; noncompliant) • Internalizing (withdrawal, depression, anxiety, obsessions, compulsions) • Cognitive/academic • Gifted or MR • Majority have low avg intelligence • 50% have concomitant learning disabilities ; also experience ADHD • Most have receptive or expressive language disorders • 50% drop out • School factors • Experience peer rejection; aggression > likely to develop conduct disorders • Need a class that values all members (strength based classroom) • Biological (genetic influence) and physiological • Environmental stressors (trauma and maltreatment) • Stressful living conditions • Child abuse • Strength-based interventions – focus on developing resiliency- self-awareness, motivation, sensitivity, problem solving • See both problems and strengths Emotional Disturbance: exhibit 1 or more of the following characteristics over a long period of time and to a marked degree that adversely affects educational performance Progress in the General Curriculum Nondiscriminatory evaluation • Inclusion • 3 x’s as many with ED served in residential settings, hospitals, homes • 6,000 incarcerated in correctional facilities • Lack of adequate support is one barrier to inclusion • Wraparound approach (health, mental health,& school services) is optimal • UDL • Adapt Assessment -- • - Self-management • (goal setting, self-monitoring, self-instruction, self-assessment, self-determination) • Augment Instruction -- • - Conflict resolution instruction (effective communication, anger management, taking another’s perspective) • Successful problem solving and decision making Prevalence • Collaboration • Community • Service learning • (Less likely to exhibit rebellion or delinquency) • Parent • Observation • Screening • Pre-referral • Referral • Evaluation • Assessment measures: IQ, achievement, behavior rating scales, direct observation, social skills, self-assessment, personality • 8 % of special education population • African-American males are over-represented in this category • Gender, ethnicity, and socioeconomic factors influence prevalence
Attributes of Teachers who work with students with emotional disturbance: Can problem solve Possess: Confidence Joy Affection Relaxed, but firm Hope, optimism, and empathy Classroom requires: Structure Predictable routines Positive praise oriented interaction with teacher, student, and others Systematic and consistent teacher response to student behavior Offer choices and give student all consequences (Note: remember to be consistent) “Tagging” Emotional or Behavioral Teachers and other professionals can HELP!
Wraparound Approach Wraparound is a philosophy of care that includes a definable planning process involving the child and family that results in a unique set of community services and natural supports individualized for that child and family to achieve a positive set of outcomes. Wraparound is an approach to implementing individualized, comprehensive services within a system of care for youth with complicated multi-dimensional problems. One population for whom wraparound has proven particularly useful is those children and adolescents with severe emotional and behavioral problems. Emerging from a strong need to reduce reliance on institutional care and to eliminate the fragmented care traditionally provided to youth who are at high risk From http://www.mentalhealth.samhsa.gov/cmhs/ChildrensCampaign/1998execsum4.asp Self-Management Self-management is any purposeful and systematic set of responses by an individual that change or maintain some aspect of that individual's behavioral repertoire. Many techniques have received attention in the self-management literature, but three main strategies have emerged and are well supported: self-monitoring self-instruction self-reinforcement (Schloss & Smith,1998). From the Article entitled, Using Countoons to teach self-monitoring skills Progressing in the General Curriculum Tips
Reverse Role tutoring (students with emotional or behavioral disorders as tutors for non-disabled peers) Improved the behavior and writing skills of the tutor Service learning Participation in in organized opportunities to meet community needs Conflict resolution Provide conflict resolution instruction to improve effective communication, anger management, and taking another’s perspective Tagging (usually used with ODD) “I’d like to discuss this at a later time, when both of us are calm > this ends the discussion and interrupts the oppositional cycle Other interventions for ODD: Providing choices Encouraging physical activity Anticipating and preventing problems Referring new students for counseling or therapy Academically Ask questions of whole class Use cooperative learning E.g think-pair-share (think about a question, pair with a peer, and share responses) Progressing in the General Curriculum More Tips
Learning Aptitude • Learning aptitude is : an individual’s capacity for altering behavior when presented with new information or experiences • Learning aptitude is assessed to gain a better understanding of the student’s ability to cope with the demands of the instructional and other environments that require changes in behavior • Evaluating learning aptitude is usually associated withIQ tests and adaptive behavior tests
IQ stands for intelligence quotient True IQ scores are measures of potential that is innate in a person False IQ scores may predict school achievement True IQ scores measure behaviors already learned in an attempt to predict future learning True The Meaning of Intelligence Tests Are the statements below True or False? • Intelligence tests mean what?
Students with mental retardation often have limits in adaptive behavior in the areas of: Social and practical skills Daily living Communication Social skills Definition: the ability to cope with the demands of the environment; includes self-help, communication, and social skills; behavior that enables the individual to “fit in” with their environment and peers What is Adaptive Behavior? Adaptation to his/her environment • So, What is adaptive behavior?
Subavg. intellectual functioning concurrently with deficits in adaptive behavior that manifest during the developmental period • Adversely affects a child’s educational performance IQ 70 and below Characteristics Progress in the General Curriculum Limits in Intellectual functioning Limits in adaptive behavior Definition • Solving problems • Thinking abstractly • Remembering information and skills • Generalization of skills from one setting to another • Decreased motivation (outer-directedness-distrusting self and looking to others) as a result of failures • Vulnerable to control by others UDL Alter curriculum w/ functional skills (e,g, applied skills, self care, health and safety, career education) Augment instruction w/ community-based instruction (relevant skills taught in community settings) or self-determination instruction • Social and practical skills • Daily living (dressing, toileting, feeding) • Communication (answer and understand) • Social skills Mental Retardation (Ch. 9 ) Research on inclusion • Twice as likely to spend time outside of general curriculum • Academic gains are more positive with greater degree of inclusion • More Socially competent and accepted • Older students experience negative consequences from inclusion • Trend to include students with MR in general education • Less receive diploma (state assessments negatively affect graduation?) Prevalence Nondiscriminatory evaluation Causes • Biomedical (e.g. chromosomal) • Social/Behavioral/educational • Exposed to lead • injuries (accidents, falls, and child abuse) • strong link b/t poverty & disability (e.g. younger mothers with 12 yrs of education or less) • 12% prenatal (before birth); 6% perinatal (during birth); 4% postnatal (after birth); 78% probable cause could not be determined • 9.6 % of special education l population • Observation • Screening • Prereferral • Referral • Evaluation • Types of assessment • IQ test, adaptive behavioral scales, direct observation, anecdotal records
Tips • Memory • Quietly repeating instructions to themselves and moving objects in a particular order as an aid to remembering a sequence of activities • Motivation • Benefit from instruction in self-determination (make choices and decisions of one’s own life free from undue external influences) • Self-determined people shape their future, they do not depend on luck (choice making, decision making, problem solving, and goal setting) • Benefits: students>> join their teachers and families in making important decisions; as adults they benefit from positive outcomes such as earning more money; have a savings or checking account; live outside of parents’ home • General • Be concrete (e.g. use of demonstration) • Visuals • Break tasks into small steps • Hands-on materials • Experiences to try things • Provide Immediate feedback
Other Health Impairment . . . means having limited strength, vitality, or alertness, including a heightened alertness to environmental stimuli, that results in limited alertness with respect to the educational environment, that—(a) is due to chronic or acute health problems such as asthma, attention deficit disorder or attention deficit hyperactivity disorder, diabetes, epilepsy, a heart condition, hemophilia, lead poisoning, leukemia, nephritis, rheumatic fever, and sickle cell anemia; and (b) adversely affects a child’s educational performance. IDEA's Definition of OHI
AD/HD:A Health Impairment • persistent pattern of inattention and/or hyperactivity-impulsivity that is more frequently displayed and severe than is typically observed in individuals at a comparable level of development
Nonverbal working memory (ability to retrieve images of the past) Difficulty with learning from previous experience > e.g. repeatedly disciplined for same mis-behavior Internalization of speech (talk to self; think about social rules) Unable to inhibit an inappropriate comment Self regulation (of affect, motivation, and arousal) Less objective, more emotional Difficulty understanding the effect of their behavior on others Lack of energy to carry out some behaviors/tasks Reconstitution Reduced capacity to be goal directed in completing tasks (difficulty taking a long-term project and breaking it down into smaller tasks> thus procrastinates and does it all last minute) Executive Functioning up close AD/HD as a disability of performance
Inattentive type (ADD) • Educators may overlook b/c they are not as disruptive; trouble with sustaining attention, easily distracted, forgetful in daily activities, internally focused; often looses things necessary for tasks or activities • Withdrawn, forgetful, a daydreamer • Withdraws from social situations • Work is incomplete, full of errors, and sloppy • Motivation is inconsistent or lacking Hyperactive-impulsive type (HD) • hyperactivity-:Often exhibits temper outbursts, Sleep problems, Talk excessively, Do not sit still (‘on the move’) , accident prone, Fidgets in seat; restless, talkative, impulsive, or easily distracted • Impulsivity: Difficulty awaiting his/her turn, May interrupt or intrude on others, may blurt out answers before questions have been completed • Typically start b/t ages 3-4 (starts before inattentive type of AD/HD) • Bursts into social situations and may be gregarious or inappropriate and annoying • Work is incomplete, full of errors, and sloppy • Motivation is inconsistent or lacking Combined type • 85% of students (most students have combined) • Features of both Hyperactive-impulsive & inattentive behaviors
Characteristics Definition Causes Russell Barkley considered father of ADHD Persistent pattern of inattention and/or hyperactivity – impulsivity • Diagnostic Criteria • Inattentive type (ADD) • Educators may overlook b/c they are not as disruptive; trouble with sustaining attention, easily distracted, forgetful in daily activities, internally focused; often looses things necessary for tasks or activities • Hyperactive-impulsive type (HD) • hyperactivity-:Often exhibits temper outbursts, Sleep problems, Talk excessively, Do not sit still (‘on the move’) , accident prone, Fidgets in seat • Impulsivity: Difficulty awaiting his/her turn, May interrupt or intrude on others, may blurt out answers before questions have been completed • Typically start b//t ages 3-4 (starts before inattentive type of AD/HD) • Combined type • 85% of students (most students have combined) • Features of both Hyperactive-impulsive & inattentive behaviors • Deficits in executive functioning (being able to process information in order to solve problems, take actions, and make decisions) • Deficits in 4 executive function areas • Nonverbal working memory • Internalization of speech • Reconstitution • Self regulation of affect, motivation, and arousal • Biological • Neurological in nature • Pre,peri,post natal • Teratogens (smoking, alcohol, drugs, exposure to chemical poisons, poor maternal nutrition, high blood pressure) • Peri/post (brain infections, complications with labor and delivery, iron deficiency anemia) • Brain differences (inability to inhibit impulses) ; lack of dopamine in some areas of the brain that regulate memory and impulsivity> thus stimulant medication given to regulate/improve executive functions • Genetics (genetic link indicates it’s a human trait) > genetic factors cause AD/HD in 80% of children and youth who experience it AD/HD (ch.8) (included under OHI) Characteristics continued . . . • Intellectual functioning & academicachievement • Usually have typical intelligence (but may also be below average as well) • 10 – 40% have a LD • 30% have a reading disability • More likely to repeat a grade, be expelled, be suspended, and receive special education • Behavioral, social and emotional characteristics • 25% have an anxiety disorder • Risk for low self-esteem, poor grades, dropping out, and conduct disorder • Higher rates of using alcohol, tobacco, and having other substance abuse issues • Conflict with parents, teachers, and peers Prevalence • Increasing dramatically • 2-9% of all children • 3 x’s as many boys as girls • Prevalence higher at preschool • Present in all ethnic groups • Latinos less likely than other students to receive an AD/HD diagnosis • 2/3 with co-existing conditions (ED, LD, SLI, gifted)
Educator's toolbox Nondiscriminatory evaluation Progress in the General Curriculum • Observation(teachers and parents observe) • Screening (classroom work products, Group intelligence tests, Group achievement tests, medical screening, vision and hearing screenings) • Prereferral (implement suggestions/intervention; the student is NOT responsive to adaptations) • Referral (referred for complete evaluation) • Nondiscriminatory evaluation procedures • Psychological evaluation (student meets DSM –IV criteria for AD/HD) • individualized IQ test • individualized achievement test • behavior rating scale • curriculum-based assessment • direct observation • Determination (has and NEEDS special education and related services) Inclusion Collaboration • UDL • Augment curriculum • Need for a stimulating curriculum • Relevance (e.g. meaning to them personally) • Novelty (presenting information in a new way) • Variety (e.g. variety of screen colors) • Choices (e.g. consider their ideas for projects) • Activity (e.g. the need to move) • Challenge (e.g. interesting, higher level thinking) • Feedback (needs external motivation) • Accommodations for ADHD • p. 223 Box 8.3 • Inclusion Tips > p. 230 Impaired social relationships Need to experience positive relationships with classmates • Team • Coach or professional organizer • Not every student qualifies for IDEA • To qualify it must adversely affect educational performance • Some get 504 (section 504 of the Rehabilitation Act of 1973) plan vs. an IEP
Educator's responsibility Stimulating curriculum • Provide an example of how you could develop a stimulating curricular environment: • Relevance (meaning to them personally) • Novelty (presenting information in a new way) • Variety(variety of screen colors) • Choices(consider their ideas for projects) • Activity(the need to move) • Challenge(interesting, higher level thinking) • Feedback (needs external motivation) ADHD
Inattentive type Difficulty working in a distracting environment Absorbing large amounts of info Transitioning from one task to another Enough time to shift from one activity to another Teach them techniques for organizing thoughts (e.g. brainstorming) and materials (e.g. tabbed notebook) Give flexible time limits (e.g. for assignments or exams) Simply tasks that have multiple steps Educator's Toolbox what do I do?
P. 223 chart (Accommodations for AD/HD) Preferential seating Extended time to complete work Ignoring inappropriate behaviors Stretch break or being able to stand while in class Reassuring and encouraging students with mood characteristics Providing daily or weekly reports to the student and parents regarding organizational tools and devices Praising student’s appropriate behavior, providing immediate feedback, and ignoring minor misbehaviors P. 222 (classroom arrangement features to minimize disruption related to hyperactivity-impulsivity) Seat student in close proximity to teacher Do not sit students with hyperactivity-impulsivity too near highly distracting areas such as windows, open doors looking into a hallway or another room, or any area with movement or potential distractions Post daily and weekly schedules Keep the schedule consistent to provide greater predictability Arrange the classroom to facilitate smooth transitions between classroom activities Interventions
Inclusion (p. 230) Teachers Typically • May overlook student (inattentive type) • May call attention to his or her isolation in front of others and force him or her to play • May be too critical or punitive (HD type) • Pull out of social situations for inappropriate behavior • Assign failing grades to the student • Send frequent notes to parents about your disappointment in their son’s or daughter’s motivation Teachers could: • Change student’s seat • Provide daily schedules • Teach the student organizational and goal-setting skills • Role play friendship skills • Use errorless learning to present stimuli and arrange prompts that will enable him or her to be successful • Use goal attainment (student may see progress and provide rewards on a periodic basis when he or she accomplishes his or her goals)
Errorless learning • Presents discriminative stimulus to the student and arranges the delivery of prompts for the student in such a way that the student gives only correct responses • Errorless learning focuses on learning that occurs without mistakes is stronger and lasts longer • Discriminative stimulus (event or environmental condition that elicits a desired response) • Stimulus acquires control over the desired response when the response is paired with a reinforcer. • Prompts are additional stimuli that increase the changes that the discriminative stimulus will elicit the desired response. Prompts may be visual, physical, or verbal • Instruction + SD (perform a task) = desired response • Instruction + Discriminative Stimulus+ prompt= desired response • Brain based learning • Teach students about their brains • Teach students how to set and attain goals • Teach students how to optimize their brainpower • Teach students their unique learning strengths (their identified preferences on ways to learn) • Create an environment conductive to brain-based learning (visual cues and reminders, hands-on activities, and music) • Improve member performance by associating and learning with emotions and sensory experiences (emotionally powerful experiences promote memorization are hands-on, and sensory based) • Teach students memory recall strategies such as mnemonic strategies (See. P.315-316) • Key word strategies (linking a keyword to a new word or concept to help remember the new material) • Pegword strategy (remember numbered or ordered information by linking words that rhyme with numbers) • Letter strategy (acronyms or a string of letters to help students remember a list of words or concepts) • http://www.ldonline.org/article/5912/