Download
1 / 29
290 likes | 425 Views
Integrated Approach to Wellness. Mary Cummins Juan Prieto. Agenda. Management System Integrated Approach to Wellness Mental health care Wellness for Life Center Interaction- Qs and As Wrap Up. What is a management system?. Describes: the way an organization does business

E N D
Integrated Approach to Wellness Mary Cummins Juan Prieto
Agenda • Management System • Integrated Approach to Wellness • Mental health care • Wellness for Life Center • Interaction- Qs and As • Wrap Up
What is a management system? Describes: • the way an organization does business • how it plans • how it executes • how it verifies the outcomes of plans • how it reviews operational status
How the organization does business • Review Corporate Philosophy and Goals • Alignment with Corporate Strategy • Global Wellbeing Services and Health Benefits Alignment • Quality criteria – person centered, effectiveness, safety, and efficiency
Quality Measures • Person Centered • This quality element focuses on the role that individual behavior and decision-making has in achieving good health outcomes and working safely • Effectiveness • This means using the best available scientific knowledge to provide specific interventions and services to those who will benefit and to avoid their use in others • Safety • This means safety at work and at home, but also safety when interacting with the health care system • Efficiency • Initiatives in efficiency seek to eliminate costly waste of resources, provide competitive cost per unit of service, and achieve affordability and fairness in cost sharing
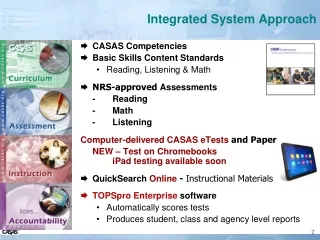
IBM Care Advocacy Model Tomorrow: Enhanced Prevention, Wellness, Treatment 2 1 3 Clinical Self Referrals SCCAP Medical/PCP GWBS Referral Health Screening Disease Management Disability • SCREENING • UBH trains all intake • (Phone/Mail/Web) • Clinical Risk • Life Change • Change Readiness • Life Cycle Issues Promotions W-3 GWBS Seminars/Fairs Adoption Lifeworks Critical Incidents Acquisitions Vendor's Web Life Status Change HRA 7 • 7NAVIGATOR • (Single Point of Entry) • Telephonic Intake • Online Live Coaching • Individual Member Web Portal • Data Driven Activation Messaging 6 4 Warm Transfers MH/SA (Clinical Mgr.) Life Balance (Case Mgr) Care Coordination Program Structured Member Support Program for Co-morbid Medical and Behavioral conditions (Depression, Anxiety, Stress and Substance Abuse) 5 • Data Driven Identification • Psychotropic Rx • Outcomes Measurement MMHC LifeSolutions No Risk Risk EAP Outcome Measures Info/Ed. Outcome Measures L M H Outcome Measures
IBM’s Care Advocacy Model Moving Care Advocacy Forward through Research • Research on outcomes, costs, and ROI for integrated behavioral health programs targeting: • High-risk medical patients • Disabled employees (GWBS) • Untreated depression and other behavioral health conditions
Outreach Products and Services Integration with Health Care Partners • Disability outreach with GWBS • Screening tool / procedure recommendations for GWBS • Referral of all targeted chronic conditions to UBH for assessment • Medical Interface Integration of behavioral and medical cases among the 5 health plan vendors and UBH • Protocols to ensure efficient coordination between medical providers and UBH • Procedures for co-management of cases • Screening tools for medical vendors and guidelines for identifying BH referrals • Disease Management Interface Interchange of Claim and UR data DM receives pharmacy data Warm transfers between DM and UBH • Integration with Lifeworks
Behavioral Health Research • Predictive modeling • Intake • Post hospitalization • Level of care forecasting • Continuing care line • Outreach program • Treatment outcome program • Care Coordination program Using Technology to Improve
Clinical Tools Align Quality & Cost Outreach Program • Substance Abuse • Offered to all members in acute treatment for substance use disorder • Requires step-down planning at admission • Follow-up appointment within 3 days of discharge • Patient outreach within 5 days of discharge • Includes family education & coordination activities • Tracks adherence and progress for one full year • Outpatient • Follow up contact within 7 days after authorization • Inpatient • Follow up contact within a day of discharge • Follow up contact within 7 days of discharge
Evaluation of the Outreach Component • Key Findings • Outpatient Services: 95% of IBM patients who received an authorization had a kept appointment compared to 85.7% for UBH book of business (p<.05). • Inpatient Services: 97% of IBM patients discharged received step-down care at any point after discharge compared to 71% for UBH book of business (p<.05). • 2004 HEDIS Quality Compass Measures: 70%. • Trend analysis completed in June 2006 replicated the above results, indicating that IBM patients outperformed UBH book of business patients on several metrics. Significant differences were found for rate of kept outpatient appointments (p<.05) and aftercare follow-up (p<.05).
Treatment Outcomes Program • Global Distress is the composite index of anxiety and depression symptoms, functional impairment, and/or impaired sense of well-being. The mean scores showed significant improvement in all domains (p<.0001). At six-months; • 64% (N=148) of IBM respondents reported no symptoms or impairment • Of those reporting residual global distress (N=73); • 32% (N=23) reported significant improvement • 18% (N=13) reported positive change • 21% (N=15) reported negative change • 30% (N=22) reported significant worsening The UBH book of business sample showed comparable results. 57% reported no symptoms or impairment. Of those who reported continuing global distress (N=245), 32% reported significant improvement, 23% reported positive change, 15% reported negative change, and 30% reported worsening. • IBM employees (N=110) reported an 88% reduction in days missed from work in the prior month, from an average of 1.89 at baseline to 0.22 at six-months (p<.05). IBM employees also reported a 54% reduction in presenteeism (work days in which productivity was ‘cut back’ due to problems) from a baseline average of 2.76 days to a six-month average of 1.27 days (p<.05). The incidence of absenteeism and presenteeism were higher in the UBH book of business sample (N=361) but within that sample, too, significant improvements were reported at 6-months; 49% reduction in absenteeism from 2.79 to 1.42 days (p<.001) and 42% reduction in presenteeism from 4.17 to 2.41 days (p<.001).
Treatment Outcomes Program • 51% of IBM respondents (N=118) reported using alcohol or drugs in 30 days prior to treatment onset. 7% (N=15) were deemed at risk for substance use disorders reporting an average of 13.6 drinks/week at baseline and 10.9 drinks/week at 6-onths, a 20% reduction which was not statistically significant. Among the UBH book of business sample, 6% (N=40) of respondents were considered at risk for substance use disorders and they reported a 40% reduction in use from an average of 13.6 drinks/weeks at baseline to 8.1 drinks/week at 6-months (p<.01). • Majority of IBM respondents (82%, N=188) reported good to excellent health at baseline (82%, N=188) and at six-months (80%, N=185). Not surprisingly, therefore, there was no measurable change in the perceptions of general health. IBM respondents did report a significant decrease in use of medical services (p<.01). At baseline 29% (N=67) reported having two or less medical services in prior six months. However, at six-months, the percentage increased to 36% (N=84) (p<.01). The UBH book of business sample reported a slight improvement in perceptions of general health (74% reported good to excellent health at baseline vs. 75% at six-months, p<.001) and reduced medical service use (29% reported one or no medical visits at baseline vs. 33% at six months, p<.01).
IBM Care Advocacy Model Tomorrow: Enhanced Prevention, Wellness, Treatment 2 1 3 Clinical Self Referrals SCCAP Medical/PCP GWBS Referral Health Screening Disease Management Disability • SCREENING • UBH trains all intake • (Phone/Mail/Web) • Clinical Risk • Life Change • Change Readiness • Life Cycle Issues Promotions W-3 GWBS Seminars/Fairs Adoption Lifeworks Critical Incidents Acquisitions Vendor's Web Life Status Change HRA 7 • 7NAVIGATOR • (Single Point of Entry) • Telephonic Intake • Online Live Coaching • Individual Member Web Portal • Data Driven Activation Messaging 6 4 Warm Transfers MH/SA (Clinical Mgr.) Life Balance (Case Mgr) Care Coordination Program Structured Member Support Program for Co-morbid Medical and Behavioral conditions (Depression, Anxiety, Stress and Substance Abuse) 5 • Data Driven Identification • Psychotropic Rx • Outcomes Measurement MMHC LifeSolutions No Risk Risk EAP Outcome Measures Info/Ed. Outcome Measures L M H Outcome Measures
Physical Activity Rebate Getting 120,000 Employees Up and Moving
Year-round support for an active lifestyle Participate on a team or alone Set activity goals Log physical activity Receive behavior change email messages Interact with fitnessprofessionals Web-based coaching IBM’s Virtual Fitness Center VFC Offerings Since 1999
Virtual Fitness Center: Successful Tool for Increasing Physical Activity Physical Activity Rebate • Join Wellness for Life Web site • Complete Physical Activity Behavior Assessment • Log physical activity on Virtual Fitness Center • Engage in physical activity • 30 minutes per day, 4 days per week for 10 of 12 consecutive weeks OR • 30 minutes per day, 2 days per week for 10 of 12consecutive weeks • plus complete 3 web-basedcoaching activities.
2006 Healthy Living Rebates Update (through August) 2005 Physical Activity Reference through August: 108K (81%) elected to participate, 82K (76%) registered on web site, and 51K (47%) earned rebate.
Evolution of Healthy Living Rebate Programs 2003 2004 2005 2006 • Non-Smokers Discount: • $11/mo. premium discount • Not smoking or smoking cessation program • Physical Activity Rebate: • $150 cash rebate • 20 min. 3 days/wk for 10 out of 12 weeks • Log activity on Virtual Fitness Center (VFC) • Smoke-Free Rebate: • $150 cash rebate • Not smoking or smoking cessation program • Physical Activity Rebate: • $150 cash rebate • 20 min. 3 days/wk for 10 out of 12 weeks • Log activity on Virtual Fitness Center (VFC) • Smoke-Free Rebate: • $150 cash rebate • Not smoking or smoking cessation program • Preventive Care Rebate: • $150 cash rebate • Complete online HRA • Set action dates for preventive screenings & health risk reduction • Review hospital quality using Web-based resources • Physical Activity Rebate: • $150 cash rebate • Option 1: 30 min. 4 days/wk for 10 out of 12 weeks • Option 2: 30 min. 2 days/wk for 10 out of 12 weeks, plus web-based coaching • Log activity on Virtual Fitness Center (VFC) • New Hire Smoke-Free Rebate: • $150 cash rebate • Not smoking or smokingcessation program
Lower Healthcare Claims Costs Seen With Moderate Levels of Physical Activity $618 Difference *2003 IBM paid medical and pharmacy claims costs. **Self-reported physical activity on 2004 IBM HRA (No response=71) (Total N=36,414 of 54,072 HRA participants matched to claims costs).
Significant health risk reduction among program participants
Higher Healthcare Claims Costs Seen with Greater Health Risk $5,810 $3,497 $2,532 *2003 IBM paid medical and pharmacy claims costs.
IBM’s Leadership Approach to Health Care • Employees can receive up to $300 in cash rebates for: • Being smoke-free or participating in a smoking cessation program • Participating in physical • activity program • Developing a health improvement plan • REBATES FOR HEALTHY CHOICES • One no-cost medical and dental option for every employee • Choice, higher benefit price tags for those needing more services • “Per-person” pricing for dependents reflects underlying costs, lower subsidy • “No coverage” cash back • EMPLOYEE-CENTERED INVESTMENT • Commitment to health care quality • Fairness in cost-sharing • Industry leading incentives to promote employee well-being • Voice for health care reform • AGGRESSIVE PURCHASING AND SUPPORT FOR HEALTH CARE REFORM • Building quality incentives into medical plans, provider relationships • Aggressive purchasing to leverage best “deals” • Working with others to improve patient safety • Reduce medical errors • Solution for the uninsured • Influence public policy: Medicare Reform, Health Care Savings Accounts FOCUS ON PREVENTION AND VALUE IN MEDICAL CARE • Free coverage for preventive visits and screenings • Deductible-free preventive and routine care • Comprehensive coverage for serious illness • Aggressive support for chronic illness • Integrated health care