Download
1 / 51
720 likes | 1.99k Views
Rhabdomyolysis: Challenges in the ICU. Leanna R. Miller, RN, MN, CCRN-CSC, PCCN-CMC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN. Rhabdomyolysis. Objectives Identify the causes of rhabdomyolysis. Describe signs and symptoms of rhabdomyolysis.

E N D
Rhabdomyolysis:Challenges in the ICU Leanna R. Miller, RN, MN, CCRN-CSC, PCCN-CMC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN
Rhabdomyolysis Objectives • Identify the causes of rhabdomyolysis. • Describe signs and symptoms of rhabdomyolysis. • Utilizing a case study, identify management strategies of a patient with renal dysfunction resulting from rhabdomyolysis.
Rhabdomyolysis • “Rhabdomyolysis was first reported in 1881, in the German literature” (Abbeele, Parker, 1985). • “Rhabdomyolysis was first described in the victims of crush injury during the 1940-1941 London, England, bombing raids of World War II” (Craig, 2006).
Rhabdomyolysis • Rhabdomyolysis accounts for an estimated 8-15% of cases of acute renal failure. • the overall mortality rate for patients with Rhabdomyolysis is approximately 5% • Rhabdomyolysis is more common in males than in females • may occur in infants, toddlers, and adolescents
Rhabdomyolysis • disintegration of striated muscle • results in the release of muscular cell constituents into the extracellular fluid and the circulation • major component released is myoglobin
Rhabdomyolysis • massive amounts of myoglobin are released the binding capacity of the plasma protein is exceeded • myoglobin is then filtered by the glomeruli and reaches the tubules, where it may cause obstruction and renal dysfunction
Rhabdomyolysis • syndrome characterized by muscle necrosis and the release of intracellular muscle constituents into the circulation • creatine kinase (CK) levels are typically markedly elevated, and muscle pain and myoglobinuria may be present
Rhabdomyolysis • severity of illness ranges from asymptomatic elevations in serum muscle enzymes to life-threatening disease associated with: • extreme enzyme elevations • electrolyte imbalances • acute kidney injury
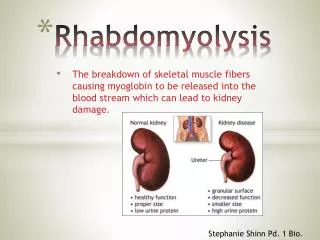
Rhabdomyolysis • Rhabdomyolysis is the breakdown of muscle fibers, specifically of the sarcolemma of skeletal muscle, resulting in the release of muscle fiber contents (myoglobin) into the bloodstream.
Rhabdomyolysis Source: (Muscle Anatomy & Structure, 2007) The sarcolemma is the cell membrane of a muscle cell. The membrane is designed to receive and conduct stimuli
Rhabdomyolysis • when muscle is damaged, a protein pigment - myoglobin is released into the bloodstream and filtered out of the body by the kidneys. • broken down myoglobin may block the structures of the kidney, causing damage such as acute tubular necrosis or kidney failure. • dead muscle tissue may cause a large amount of fluid to move from the blood into the muscle, leading to hypovolemic shock reduced blood flow to the kidneys.
What Causes Rhabdomyolysis • may result from a large variety of diseases, TRAUMA, or toxic insults to skeletal muscle • hereditary myopathies
Rhabdomyolysis • Causes • trauma • burns • compression syndrome • infection • seizures • heat intolerance • heat stroke
Rhabdomyolysis • Causes • vascular occlusion • prolonged shock • electrolyte disorders • drugs (cocaine, alcohol, statins, amphetamine) • low phosphate levels • shaking chills
Rhabdomyolysis • Clinical Manifestations • muscle tenderness • myalgias • muscle swelling & weakness • DIC • color of urine
Rhabdomyolysis • Additionally some possible symptoms include: • Overall fatigue • Joint pain • Seizures • Weight gain
Rhabdomyolysis • Diagnosis • an examination reveals tender or damaged skeletal muscles • Creatine Phosphokinase (CK) levels are very high • serum myoglobin test is positive • serum potassium may be very high
Rhabdomyolysis • serum CK begins to rise within 2 to 12 hours following the onset of muscle injury and reaches its maximum within 24 to 72 hours • decline is usually seen within three to five days of cessation of muscle injury
Rhabdomyolysis • CK has a serum half-life of about 1.5 days and declines at a relatively constant rate of about 40 to 50 percent of the previous day’s value • patients whose CK does not decline as expected, continued muscle injury or the development of a compartment syndrome may be present
Rhabdomyolysis • Diagnosis • Urinalysis may reveal protein and be positive for hemoglobin without evidence of red blood cells on microscopic examination • Urine myoglobin test is positive
Rhabdomyolysis • Urine Myoglobin • visible changes in the urine only occur once urine levels exceed from about 100 to 300 mg/dL • can be detected by the urine dipstick at concentrations of only 0.5 to 1 mg/dL • half-life of only two to three hours, much shorter than that of CK. • rapidly excreted and metabolized to bilirubin, serum levels may return to normal within six to eight hours
Rhabdomyolysis • Lab Values • elevated muscle enzymes (CK) • hyperkalemia • hyperphosphatemia • hypocalcemia
Rhabdomyolysis • Complications • Kidney damage • Acute renal failure • Hyperkalemia • Cardiac arrest • Disseminated Intravascular Coagulation • Compartment syndrome
Rhabdomyolysis • Treatment • volume replacement • treat electrolyte abnormalities • protect renal perfusion • alkalinization of urine • fasciotomy
Rhabdomyolysis • early and aggressive fluids (hydration) may prevent complications by rapidly remove myoglobin out of the kidneys. • administer isotonic crystalloid fluids (Normal Saline or Lactated Ringer’s) • give as much fluid as you would give a severely burned patient.
Rhabdomyolysis studies of patients with severe crush injuries resulting in Rhabdomyolysis suggest that the prognosis is better when prehospital personnel provide FLUID RESUCITATION!
Rhabdomyolysis • medicines that may be prescribed include diuretics and sodium bicarbonate. • hyperkalemia should be treated if present • kidney failure should be treated as appropriate
Rhabdomyolysis • if urinary flow is >20 mL/hour add mannitol to the intravenous alkaline solution providing an increase in urine output is demonstrated following a test dose • suggested test dose is 60 mL of a 20 percent solution of mannitol administered intravenously over three to five minutes
Rhabdomyolysis • if urine output increases by at least 30 to 50 mL/h above baseline levels in response to the test dose, 50 mL of 20 percent mannitol (1 to 2 g/kg per day [total, 120 g], may be given at a rate of 5 g/hour. • mannitol is contraindicated in patients with oliguria
Rhabdomyolysis • The outcome varies depending on the extent of kidney damage. Source: Silberber, 2007
Rhabdomyolysis • Renal Failure Index (RFI) • RFI = UNa x SCr/UCr • Intrepretation • RFI < 1 (prerenal failure) • RFI > 1 (intrarenal failure)
Rhabdomyolysis • Fraction Excreted Sodium (FENa) • FENa = Una X PCr / Pna X Ucr x 100 • Intrepretation • FENa < 1 (prerenal failure) • FENa > 1 (intrarenal failure)
Rhabdomyolysis • Renal Failure Index (RFI) • RFI = UNa x SCr/UCr • Example • RFI > 1 • UNa>40 mEq/L • FENa > 2-3% • UCr/SCr<20
Rhabdomyolysis • Renal Biomarkers • Urine interleukin – 18 (IL – 18) • Urine or blood NGAL • neutrophil gelatinase – associated lipocalin Increase 24 to 48 hours earlier than creatinine
Rhabdomyolysis Intrinsic • Diagnostics • BUN/Creatinine ratio • RFI/FENa • urinalysis
Rhabdomyolysis Treatment • underlying cause • prevention on injury • high risk patient • hydration • limit exposure
Rhabdomyolysis Management Principles • maintain fluid balance • manage hyperkalemia • glucose & insulin • sodium bicarbonate • calcium gluconate • albuterol
Rhabdomyolysis Clinical Manifestations • hyperkalemia • hypocalcemia • hypermagnesemia • hyperphosphatemia • acid – base imbalance
Rhabdomyolysis • hypocalcemia occurs in up to two-thirds of patients with significant rhabdomyolysis • increase in serum phosphate • deposition of calcium phosphate into injured muscle • decreased bone responsiveness to parathyroid hormone
Rhabdomyolysis Management Principles • control hypertension in presence of encephalopathy • bicarbonate for severe acidosis (pH < 7.2) • manage anemia
Rhabdomyolysis Treatment • Replacement Therapies • acidosis • HCO3 < 10 mEq/L • K+ > 6.5 mEq/L • need high protein diet • deteriorating
Rhabdomyolysis Treatment: • Types • hemodialysis • continuous renal replacement therapy
Rhabdomyolysis Treatment • fluid balance • anticoagulation • prevent clotting • prevent blood loss • ultrafiltration
Rhabdomyolysis Case Study • 20 – year old male with friends “doing drugs – cocaine” • police break up party – male runs from police but collaspes – states legs became so weak that he fell • admitted to ED – lower extremity weakness and severe pain in legs
Rhabdomyolysis Case Study
Rhabdomyolysis Case Study
Rhabdomyolysis Case Study