Download
1 / 81
900 likes | 1.32k Views
Chapter 4. Tissue Response to Injury: Inflammation, Swelling, and Edema. Inflammation. The local response of the body to an irritant Purpose Defend the body against alien substances Dispose of dead and dying tissue so repair can take place. Cardinal Signs of Inflammation. Rubor: redness

E N D
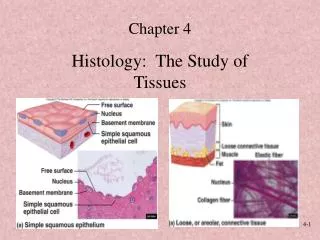
Chapter 4. Tissue Response to Injury: Inflammation, Swelling, and Edema
Inflammation • The local response of the body to an irritant • Purpose • Defend the body against alien substances • Dispose of dead and dying tissue so repair can take place
Cardinal Signs of Inflammation • Rubor: redness • Calor: heat • Edema: swelling • Dolor: pain • Funca laesa: functional loss Each of these signs will occur to some degree when tissue is injured and the body responds with the inflammatory process.
Common Misconceptions of Inflammation • Do you need to limit or eliminate inflammation? • No. Inflammation is necessary. • Repair will not occur without inflammation. • You cannot eliminate inflammation. • You can only minimize the signs of inflammation.
Common Misconceptions of Inflammation (cont.) • Swelling, edema, and inflammation are synonymous • Swelling and edema occur during inflammation. • Edema and swelling are not the same. • All edema causes swelling, but not all swelling is caused by edema.
Phases of Inflammation • Inflammation consists of sequential and overlapping events. • Primary injury • Ultrastructural changes • Chemical mediation • Hemodynamic changes • Metabolic changes • Permeability changes • Leukocyte migration • Phagocytosis
Primary Injury • Any occurrence that impairs tissue structure or function • Most sports injuries are caused by • Macrotrauma (impact or contact) • Microtrauma (overuse, cyclic loading, or friction) • There are many other types of injury, each of which results in the same basic inflammatory reaction. • Other examples?
Primary Injury (cont.) • Other causes of injury include • Physical agents (trauma, burns, radiation) • Metabolic processes (hypoxia) • Biological agents (bacteria, viral, parasitic, infection) • Chemical agents (acids, gasses, organic solvents, endogenous chemicals) • Endogenous chemicals • Normal secretions • In abnormal locations (gout) • In increased quantity in a normal location (stomach ulcers) • The magnitude after each phase varies according to the causative agent
Cellular membrane is disrupted and eventually breaks down. Contents spill out into the extracellular spaces, thereby killing the damaged cell. Two causes Direct Trauma (primary injury) Indirect Hypoxia (oxygen deficiency) Enzymes (chemicals) In cells adjacent to the primary injury Ultrastructural Changes
Ultrastructural Changes (cont.) • Occur as a direct result of trauma (primary injury) and indirectly as a result of hypoxia (secondary injury) • We will discuss this in more detail later in this chapter (see “Orthopedic Injury Model”).
Lysosome Supplies chemicals that digest foreign material within the cell and gets rid of it. If the membrane of the lysosome ruptures, its contents will attack and digest other material. Ultrastructural Changes (cont.)
Chemical Mediation • Histamine, bradykinin, and other chemicals • Modify and regulate the rest of the inflammatory response to: • Neutralize the cause of the injury • Remove cellular debris so repair can take place
Hemodynamic Changes • Arteries dilate, increasing blood flow to the injured area. • However, blood vessels that were previously inactive open, so blood flow through individual vessels decreases. • Slowing of blood flow is necessary, so WBCs can move to the margins.
Hemodynamic Changes (cont.) • Leukocytes • Marginate • Tumble along the vessel wall • Adhere to the vessel wall near an opening
Hemodynamic Changes (cont). • Leukocytes begin passing though the vessel wall.
Metabolic Changes • ↓ Energy • ↓ Oxygen, causes cell to switch to anaerobic metabolism • Membrane functions slow down. • Sodium pump maintains the concentration of intracellular sodium at a very low level.
Metabolic Changes (cont.) • ↑ Sodium concentration in cell and organelles • ↑ Water in cell • Cells swell and burst • ↑ Intracellular acidosis (lactic acid) • Membrane attacked • Lysosome digests cell.
Permeability Changes • Histamine and bradykinin increase the permeability of small blood vessels. • The endothelial cells contract, pulling away from each other. • Gaps are left, through which the WBCs can move out of the vessel and to the injury site.
Leukocyte Migration • WBCs adhere to the endothelium (vessel wall) and/or to other white blood cells. (Reprinted with permission from McLeod I. Inflammation. Kalamazoo, MI: Upjohn, 1973.)
Leukocyte Migration (cont.) • WBCs move out of the vessel by squeezing through the endothelial gaps. • Neutrophils first, then larger macrophages (Reprinted with permission from McLeod I. Inflammation. Kalamazoo, MI: Upjohn, 1973.)
Leukocyte Migration (cont.) • Neutrophils • Macrophages
Leukocyte Migration (cont.) • Neutrophils • Travel fast and arrive at the injury site first • Provide the first line of defense • When they die, they release chemical mediators that attract macrophages. • Death of neutrophils results in a large concentration of chemical mediators released by the cells.
Leukocyte Migration (cont.) • Macrophages • Live for months • Long-lasting second line of defense • Release potent enzymes that may destroy connective tissue, thus adding to the injury • Release chemical mediators that may prolong inflammation • Release factors that aid in healing • Secrete proteins that are important in defense mechanisms
Phagocytosis • Digestion of cellular debris and other foreign material into pieces small enough to be removed from the injury site
Chronic Inflammation • Results from microtrauma but does not necessarily involve an inflammatory reaction • Example: clinically diagnosed Achilles tendinitis and patellar tendinitis in which there is no evidence of an inflammatory reaction • Structural disruption and microvascular damage may occur (causing pain and other symptoms) before the classic inflammatory process is set into action.
Orthopedic Injury Model • What happens when a muscle is pulled or an ankle is sprained? • Just put an ice bag on it, right? • WRONG. • This is overly simplistic. • Techniques must be based on sound theory if they are to be developed and improved. • It is essential to understand the body’s response to injury.
Orthopedic Injury Model (cont.) • Example: typical tissue undergoing a typical muscular injury • Used to illustrate inflammation in relation to orthopedic injuries
Orthopedic Injury Model (cont.) • Normal tissue • Cells • Two blood vessels (A, B) • Two nerves (1, 2)
Orthopedic Injury Model (cont.) • Contusion with injury to: • Three cells • Nerve 1 • Blood vessel B
Orthopedic Injury Model (cont.) • Immediate ultrastructural change • Local nerves and blood vessels may be disrupted or broken. • This damage is called primary traumatic damage.
Orthopedic Injury Model (cont.) • Hemorrhage • Few minutes only (usually) • Clot forms, stopping hemorrhage. • Pain, from damaged nerve • Hematoma forms.
Orthopedic Injury Model (cont.) • Pain, from damaged nerve • Muscle spasm and more pain • Inhibition of muscular strength, range of motion, etc. • Body attempts to protect itself by splinting the area, thus preventing aggravation of injury.
Orthopedic Injury Model (cont.) • The damaged cells release chemical mediators as a signal to the body that an injury has taken place. • Extravascular hemorrhage occurs from broken blood vessels. • Swelling occurs. Injury site
Orthopedic Injury Model (cont.) • Fibrin forms into strands, creating a network somewhat like a fishnet. • This net captures circulating platelets. • A plug forms to seal the damaged vessel.
Orthopedic Injury Model (cont.) • Chemical mediators released from dying cells cause • Hemodynamic changes • Permeability changes • Leukocyte (white cell) migration
Orthopedic Injury Model (cont.) • Secondary enzymatic injury begins.
Orthopedic Injury Model (cont.) • Hemodynamic changes • Blood flow slows down OR • Blood flow ceases • Tissue oxygen decreases • Hypoxia • Metabolic changes • Secondary hypoxic injury soon seen No flow
Orthopedic Injury Model (cont.) • Phagocytosis • Free protein • Causes edema
Orthopedic Injury Model (cont.) • Secondary hypoxic injury begins. • Secondary enzymatic injury continues.
Orthopedic Injury Model (cont.) • Phagocytosis and secondary injury continue.
Orthopedic Injury Model (cont.) • Pressure on undamaged nearby pain fibers cause additional • Pain • Muscle spasm and inhibition
Orthopedic Injury Model (cont.) • Total injury: • Primary injury (yellow) • Secondary injury
Orthopedic Injury Model (cont.) • The inflammatory response is not all positive. • Example • Slowed blood flow in the vessels on the periphery of an injury and decreased blood flow from the damaged vasculature result in less oxygen to the cells. • If prolonged, secondary hypoxic injury occurs. • The total amount of damaged tissue is increased, and more debris is added to the hematoma.
Secondary Injury Model • Body’s response to tissue damaged by trauma (primary injury) leads to further tissue damage, known as secondary injury. • Two separate mechanisms result in secondary injury: • Enzymatic • Hypoxia
Decreased Metabolism Theory In normal tissue O2 needed O2 available
O2 needed O2 available Decreased Metabolism Theory (cont.) After injury
Decreased Metabolism Theory (cont.) After injury and cryotherapy O2 needed O2 available