Download
1 / 49
490 likes | 635 Views
Molecular Genetics. The Human Genome: Biology and Medicine. Introduction Basic Genetic Mechanisms Eukaryotic Gene Regulation The Human Genome Project Test 1 Genome I - Genes Genome II – Repetitive DNA Genome III - Variation Test 2 Monogenic and Complex Diseases Finding ‘Disease’ Genes

E N D
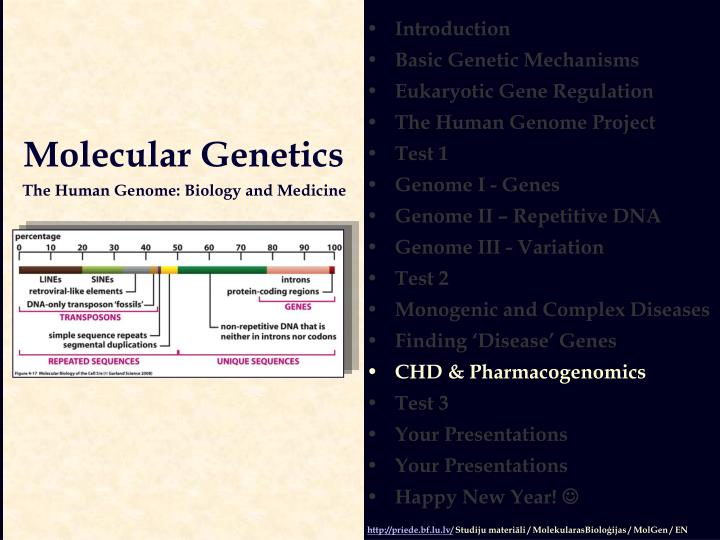
Molecular Genetics The Human Genome: Biology and Medicine • Introduction • Basic Genetic Mechanisms • Eukaryotic Gene Regulation • The Human Genome Project • Test 1 • Genome I - Genes • Genome II – Repetitive DNA • Genome III - Variation • Test 2 • Monogenic and Complex Diseases • Finding ‘Disease’ Genes • CHD & Pharmacogenomics • Test 3 • Your Presentations • Your Presentations • Happy New Year! http://priede.bf.lu.lv/ Studiju materiāli / MolekularasBioloģijas / MolGen / EN
Coronary Heart Disease (CHD) Nature Rev. Genetics (2006) 7, 163.
Endothelial Injury Inflammation Lipids + CHRONIC INFLAMMATION ATHEROSCLEROTIC PLAQUE ‘Response-to-Injury’ hypothesis
ox Lipoproteins Hypertension Elevated Homocysteine AGEs (Advanced Glycosilation End products) ROS (Reactive Oxygen Species) Infections Genetic alterations Endothelial Dysfunction Inflammation Lipids + EndothelialInjury CHRONIC INFLAMMATION Inflammation Lipids + ATHEROSCLEROTIC PLAQUE ‘Response-to-Injury’ hypothesis Possible causes
Endothelial Dysfunction in Atherosclerosis Ref.: Ross R (1999) NEJM, 340, 115-126.
Migration of leukocytes into the artery wall L-selectin Integrins PECAM-1 VCAM: vascular cell-adhesion molecule ICAM: intracellular cell-adhesion molecule PECAM: platelet endothelial cell-adhesion molecule MCP: monocyte-chemoattractant protein M-CSF: monocyte colony-stimulating factor Modified from Li AC & Glass CK (2002) Nature Medicine, 8, 1235-1242.
Atherosclerosis and familial hypercholesterolemia Life The Science of Biology, 7th Edition
Fatty-Streak Formation in Atherosclerosis Ref.: Ross R (1999) NEJM, 340, 115-126.
The foam-cell paradox Steinberg D (2002) Nature Medicine, 8, 1211-1217.
Formation of an Advanced, Complicated Lesion of Atherosclerosis Ref.: Ross R (1999) NEJM, 340, 115-126.
Yet, plaques may substantially differ one from another. Why - ??? Modified from Libby P & Aikawa M. (2002) Nature Medicine, 8, 1257-1262.
Vulnerable plaques tend to rupture: Acute Coronary Syndrome plaque rupture
e.g., Myocardial Infarction Thrombus Coagulation factors Artery Rupture Matrix Metalloproteinases PLAQUE Modified from Benitez RM (1999) Hosp Pract. 34, 79
By the way: study and you will live longer (or happier); perhaps marry Marenberg M. E. et al. (1994) Genetic Susceptibility to Death from Coronary Heart Disease in a Study of Twins. N Engl J Med 1994; 330:1041-1046. BackgroundA family history of premature coronary heart disease has long been thought to be a risk factor for coronary heart disease. Using data from 26 years of follow-up of 21,004 Swedish twins born between 1886 and 1925, we investigated this issue further by assessing the risk of death from coronary heart disease in pairs of monozygotic and dizygotic twins. Conclusions Our findings suggest that at younger ages, death from coronary heart disease is influenced by genetic factors in both women and men. The results also imply that the genetic effect decreases at older ages. What is the most common genetic risk factor of CHD?
Development of coronary heart disease (CHD) is thought to be influenced by > 100 genes Candidate genes for genetic susceptibility to CHD: late stages of lesion formation
Receptors Enzymes Ion channels Lipoproteins Coagulation factors Cell-cycle control Signal transduction drug ABSORPTION METABOLISM Drug Metabolising Enzymes Drug Transporters Drug TARGETS DISEASE- ASSOCIATED pathways ELIMINATION DISTRIBUTION Pharmaco- KINETICS Pharmaco- DYNAMICS Individual Drug Response ADR Desired drug effect
PHARMACOGENETICSGENOMICS One of the most striking features of modernmedicinesis howoftentheyfail to work.Even when they do work, they are often associated with serious adverse reactions.Goldstein DB (2003)Pharmacogenomics in the Laboratory and the Clinic. NEJM 6, 553. 1. .
Moreover, for some patients, medicines turn out to be toxic or even lethal Adverse Drug Reaction (ADR) - any noxious, unintended, and undesired effect of a drug, which occurs at doses used in humans for prophylaxis, diagnosis, or therapy (WHO definition) ADR-In: an ADR occurring in patients while in the hospitalADR-Ad: an ADR causing admission to the hospital Lazarou J et al. (1998) Incidence of Adverse Drug Reactions in Hospitalized Patients. A Meta-analysis of Prospective Studies. JAMA279, 1200-1205.
Adverse reactions are characteristic to many widely used drugs JAMA (2001) 286, 2270-2279.
The adverse reactions often are ‘lethal’ to drugs themselves & many more Need AC et al. (2005) Priorities and standards in pharmacogenetic research. Nature Genetics37, 671-681.
PHARMACOGENETICSGENOMICS Reducing ADRs Bio-equivalent dosage Meisel C et al. J Mol Med (2003) 81, 154. Annu. Rev. Genomics Hum. Genet. 2001. 2:9-39. Industry: development ADR-free drugs
Metabolism converts • Drugs to metabolites that are more water soluble and thus more easily excreted • Prodrugs into therapeutically active compounds Metabolism is classified • Phase I - transformation reactions • ox, red, hydrolysis... • Phase II - conjugation reactions • acetylation, methylation... Weinshilboum R (2003) NEJM 348, 529
A consequence of poor metabolism of a drug (normal) dose dose Molecular interventions (2003) 3, 194-204.
Contribution of individual enzyme systems to metabolism of currently marketed drugs Cytochromes P450 The AAPS Journal (2006) 8, E101.
Phase I metabolism and major human P450s Molecular Interventions (2003) 3,194-204.
Major molecular mechanisms that can result in altered human drug metabolism Ingelman-Sundberg Met al (1999) TiPS20, 342-349.
Genotype–phenotype relationships of the CYP2D6 polymorphism(the ‘debrisoquin polymorphism’)
In reality, however “...35-50 million people in Europe could be considered as ‘forgotten’ with respect to 20-30% of all drugs that are metabolised by CYP2D6”.
There are striking differences in the types and frequences of alleles among different populations Modified from Ingelman-Sundberg M et al (1999) TiPS 20, 342-349.
Pharmacogenetics of Thiopurine S-Methyltransferase (TPMT) • 6-mercaptopurine (6MP) • a powerful cell-killing compound to cure leukemia in children • TPMT • methylates & inactivates 6MP • activity of enzyme varies • 1/300 homozygous • Tests • TPMT activity in red blood cells • genotyping Ref: Weinshilboum R (2003) NEJM348, 529.
Fibrinogen receptor - GPIIb/IIIa[PlA1/A2 polymorphism (C1565T; Leu33Pro)of GPIIIa gene] eg, Abciximab Yeghiazarians Y et al. (2000) Unstable Angina Pectoris. NEJM342, 101-114.
STATINS Acetyl CoA • Cholesterol biosynthesis • more than 30 enzymes • HMG-CoA • 3-hydroxy-3-methyl-glutaryl-CoA • HMG-CoAreductase • rate-limiting enzyme • Statins • inhibit HMG-CoAreductase • Results • decreased cholesterol biosynthesis • induction of LDL receptor HMG-CoA Cholesterol biosynthesis • more than 30 enzymes HMG-CoA • 3-hydroxy-3-methyl-glutaryl-CoA HMG-CoA reductase • rate-limiting enzyme Statins • inhibit HMG-CoA reduktase Results • decreasedcholesterol biosynthesis • induction of LDL receptor HMG-CoA reductase Mevalonate Cholesterol Lipoproteins Bile acid synthesis Membrane biogenesis Steroide hormones Atherosclerosis
<30% - HDL (T) >30% - HDL (TT) CETP gene B1/B2 polym. B1 >CETP and <HDL-C than B2 B1 - promotes atherosclerosis & good response to statins B2 - no & poorer, respectively
PHARMACOGENETICSGENOMICS Etiology-specific drugs Industry: enhancing drug discovery and development.
Development of coronary heart disease (CHD) is thought to be influenced by > 100 genes Candidate genes for genetic susceptibility to CAD: the early stages of lesion formation
Individual response to drugs is a complex trait Pharmacogenetic profiles CYP2C9 + SCN1A 3*/ 3* + G/G – 250mg 1*/3* + A/G – 297mg 1*/ 1* + A/A – 377mg PNAS (2005) 102,5507-5512 Phenytoin – an antiepileptic drug CYP2C9 3* allele – altered substrate specificity SCN1A – encodes the a-subunit of sodium channel; polymorphism in a 5’ splice site