Download
1 / 61
610 likes | 628 Views
Tools of the Trade. Ambulatory Blood Pressure Monitoring. Pre-Quiz. If there was only one thing from your ABP report that you could find out, what would it be?. Outline. Rationale Instrumentation and Technique Methods of Analysis Common Parameters Diagnostic & Prognostic Utility

E N D
Tools of the Trade Ambulatory Blood Pressure Monitoring
Pre-Quiz • If there was only one thing from your ABP report that you could find out, what would it be?
Outline • Rationale • Instrumentation and Technique • Methods of Analysis • Common Parameters • Diagnostic & Prognostic Utility • Thoughts on how we use ABPM here
Why ABPM? • BP is a 24/7 parameter • BP has circadian rhythm and variability • Single Office measurements generally higher than true BP
ABPM Advantages • No observer bias • Better correlation with end-organ damage • 24 hr
Recommended Indications for ABPM CMS WHO JNC-7 White-Coat Hypertension White-Coat Hypertension Resistant HTN … yet the FDA won’t approve a new BP med without ABPM data … Unusual BP Variability Low Risk Office HTN Hypotensive symptoms while on BP meds Episodic Hypertension Autonomic Dysfunction
Other Practical ABPM uses Timing of Medications Prognosis Documenting Efficacy of BP meds
Devices • ~ 20 different devices on market • Daytime q 20 m, Night q 30-60 m • Two Types • Oscillometric • reliable MAP • algorithm for SBP & DBP • Auscultatory • More accurate SBP & DBP • R-wave gating • Prone to noise interference
Technical Limitations • Devices and Algorithms not validated before placement on market • Devices not validated in children • Watchdog Groups • British Hypertension Society (BHS) gives Grades • B or C for SBP • C or D for diastolic
Proven Feasible in Kids in 1991 • Ron Portman tested it on 95 Fifth Graders (J Pediatr, 1991) • Success & Tolerability Age & BP
So Many Parameters • Technical • % Successful Readings • Blood Pressure • Mean BP • Summary, Day, Night • BP Load • Variability • Dipping • Rhythm • Cosinor Analysis • Others • Mean HR • Pulse Pressure
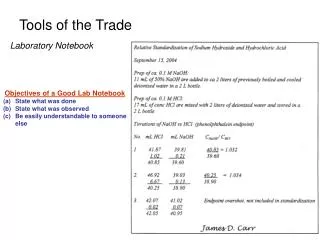
Technical Quality • > 80% of successful readings considered good • Used as standard in pediatrics as well1 • Repeat BP 3 min after an error increased success from 77% to 89%2 • Lurbe, Am J Hypertens, 1999 • Portman, J Pediatr, 1991
Mean Measurements • 90%le of SBP and DBP from JNC-7 • Do you adjustment for nighttime?
Load • 1st defined 1991 (Zachariah, JAMA) • % of readings (not time) above threshold • 35% for SBP / 25% DBP is 95%le for healthy children • 40% used in pediatric NIDDM study • 50% cutoff associated with LVH (Sorof, Hypertension 2002)
Beyond the LoadThe Hyperbaric Index & Microthresholds2 • Hermida, Blood Press Monit, 1999 • Hermida, Biomed Instr Tech, 1996
Dipping • ~ 10% decrease in BP while asleep • Probably the most important parameter • Less prominent in Black pts • Potential disrupted sleep does not influence nighttime BP’s • Reverse Dipping and Super-Dipping also described • Dipping occurs during the siesta
Variability Issues • Different sleep times for each person • Diary needed • Cultural considerations (siesta) • Exclusion of “transitional periods”
Phase Amplitude Periodicity Beyond Dipping:Cosinor Analysis f(t) = M + A.Cos(2t/24) + B.Sin(2t/24)
ABPM Parameters & Outcomes • Outcomes • LVH • CKD Progression • Microalbuminuria & Protein Excretion Rate • Cardiovascular Events • Transplant Function
ABPM and LVHAdults • ADPCKD • IgAN • NIDDM • CKD • Glomerulonpehritis • HTN with proteinuria • Kidney Transplant Patients
ABPM and CKD • Most prevalent BP abnormalities • nocturnal (sleep) period hypertension • nondipping blood pressure pattern (2/3’s) • Mean BP and Load correlates with LVH • Abnormal patterns linked to • Protein excretion • More rapid progression • CV damage and events
ABPM and ESRD • Lingens: pediatric HD patients. ABP reclassified 1/3 of HTNive’s as normotensive, 1/3 normo as HTN • Sorof. Casual BPs in pediatric HD patients had errors of –17 to 27 % for SBP
ABPM & Pediatric Renal Transplant • Lingens, 1996 • 30% had non-dipping • Sorof, 2000 • High SBP loads & 25% had reverse dipping • Calzolari, 1998 • Mean BP, Day and Night BP correlated with LVMI • Lingens, 1997 • 9/16 were wrongly classified as hypertensive by office BP
ABPM & Renal Scarring • Patzer, J Pediatr, 2003
ABPM & Adolescent NIDDM • Khan • 42% had non-dipping • Holl • n=342 • Reduced dipping compared to controls • Young • Hgb A1C inversely correlated with dipping
ABPM & Pediatric Proteinuria • Ettinger, 2005 • Higher SBP Load in those with mAlb • Garg: • Higher mean BP in those with mAlb • BP Load proportional to amount of proteinuria • Sochett • diabetics with microalbuminuria had higher • mean BP • night BP • non-dipping • BP load
Who Sleeps @ this time? Dipping? 131-121/131 = 7.6%
So…. • Intuitively better measure of BP • Wealth of information • Analysis methods lag behind technology
JHH ABPM Recommendations • Use • New patients: Low-risk hypertensive adolescents • Documenting treatment efficacy (e.g. transplant patients) • Thresholds • Continue to use JNC-7 BPs as thresholds • No nighttime adjustment of thresholds for load determination • Load • Customize sleep times for each patient • Use lower load thresholds (40%) based on normative data • Customize software to calculate Dipping