Download
1 / 58
600 likes | 781 Views
Diagnosis of Thyroid Disorders. William Harper, MD, FRCPC Endocrinology & Metabolism Assistant Professor of Medicine, McMaster University www.drharper.ca . Case 1. 31 year old female Somalia Canada 3 years ago G2P1A0, 11 weeks pregnant Well except fatigue Hb 108 , ferritin 7

E N D
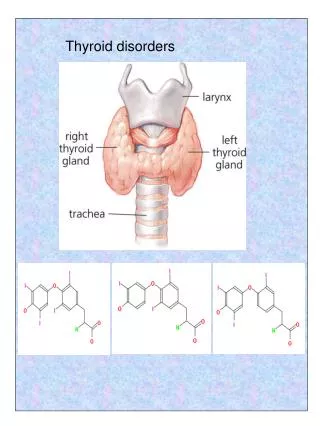
Diagnosis of Thyroid Disorders William Harper, MD, FRCPC Endocrinology & Metabolism Assistant Professor of Medicine, McMaster University www.drharper.ca
Case 1 • 31 year old female • Somalia Canada 3 years ago • G2P1A0, 11 weeks pregnant • Well except fatigue • Hb 108, ferritin 7 • TSH 0.2 mU/L, FT4 7 pM • Started on LT4 0.05 TSH < 0.01 mU/L FT4 12 pM, FT3 2.1 pM
Case 1 • How would you characterize her hypothyroidism? • What are the ramifications of pregnancy to thyroid function/dysfunction?
TSH Low High FT4 & FT3 FT4 Low Low High High Central Hypothyroid 1° Thyrotoxicosis 1° Hypothyroid If equivocal 2° thyrotoxicosis RAIU TRH Stim. • Endo consult • FT3, rT3 • MRI, α-SU MRI, etc.
TRH Stimulation test A) 1° Hypothyroidism B) Central Hypothyroidism C) Euthyroid D) 1° Thyrotoxicosis
Case 1 • GH, IGF-1 normal • LH, FSH, E2, progesterone, PRL normal for pregnancy • 8 AM cortisol 345, short ACTH test normal • MRI: normal pituitary • TGAB, TPOAB negative • LT4 increased until FT4 in hi-normal range • Normal pregnancy, delivery, baby, lactation • Considering TRH stim once done breast-feeding
Thyroid Tests • Thyroid Function • Iodine Kinetics • Thyroid Structure • FNA • Thyroid Antibodies • Thyroglobulin
Normal Daily Thyroid Secretion Rate: T4 = 100 ug/day T3 = 6 ug/day ( ratio T4:T3 = 14:1 ) T4 Protein* binding + 0.03% free T4 85% (peripheral conversion) T3 Protein* binding + 0.3% free T3 15% (10-20x less than T4) * TBG 75% TBPA 15% Albumin 10% Total T4 60-155 nM Total T3 0.7-2.1 nM T3RU/THBI 0.77-1.23
Thyroid Function Tests TSH 0.4 –5.0 mU/L Free T4 (thyroxine) 9.1 – 23.8 pM Free T3 (triiodothyronine) 2.23-5.3 pM
TSH Assay(0.4-5 mU/L) • Early RIA < 1.0 mU/L • Thyrotoxicosis / 2º hypothyroidism • Unable to detect lower range of normal • Monoclonal SEN < 0.1 mU/L • Super SEN < 0.01 mU/L
Case 1 • How would you characterize her hypothyroidism? • What are the ramifications of pregnancy to thyroid function/dysfunction?
Thyroid & Pregnancy: Normal Physiology • Increased estrogen increased TBG • Higher total T4, T3 (normal FT4, FT3 if thyroid gland working properly) • hCG peak end of 1st trimester, weak TSH agonist so may cause slight goitre • Fetal thyroid starts working at 11 wks • T4 & T3 do NOT cross placenta (or do so minimally) • Do cross placenta: PTU, MTZ, TSH-R Ab (stim or block) • MTZ aplasia cutis scalp defects
Thyroid & Pregnancy: Hypothyroidism • Will need ~ 25% increase in LT4 during pregnancy due to increased TBG levels • Risks: increased spont abort, HTN, preterm pregnancy, 7 IQ points for fetus (NEJM, 341(8):549-555, Aug 31, 2001)
LT4 dose adjustment in Pregnancy:Need TSH at baseline & q2mos while pregnantStarting LT4: 2 ug/kg/d and check TSH q4wk until euthythyroid
Thyrotoxicosis & Pregnancy • Risks: fetal anomalies, spont abort, preterm labor, fetal hyperthyoridism, thyroid storm in labor • No RAI ever • Rx options: ATD or 2nd trimester thyroidectomy • PTU drug of choice (avoid MTZ due to scalp defects) • Aim to keep FT4 levels in hi normal range • OK to breast feed on PTU as does not go into breast milk
Postpartum Thyroiditis • 5% (3-16%) postpartum women (25% T1DM) • Up to 1 year postpartum (most 1-4 months) • Lymphocytic infiltration (Hashimoto’s) • Postpartum Exacerbation of all autoimmune dx • 25-50% persistant hypothyroidism • Small, diffuse, nontender goitre • Transiently thyrotoxic Hypothyroid
Postpartum Thyroiditis • Rx: • Hyperthyroid symptoms: atenolol 25-50 mg od • Hypothyroid symptoms: LT4 50-100 ug/d to start • Adjust LT4 dose for symptoms and normalization of TSH • Consider withdrawal at 6-9 months (25-50% persistent hypothyroid, hi-risk recur future preg)
Postpartum & Thyroid • Postpartum depression • When studied, no association between postpartum depression/thyroiditis • Overlapping symtoms, R/O thyroid before start antidepressents • Screening for Postpartum Thyroiditis HOW: TSH q3mos from 1 mos to 1 year postpartum? WHO: • Symptoms of thyroid dysfn. • Goitre • T1DM • Postpartum thyroiditis with prior pregnancy
Case 2 • 47 year old female • Concerned about weight gain over past 15 years (15 lbs). Otherwise asymptomatic • BMI 25, Thyroid: 40 gm, rubbery firm. • TSH 6.7 mU/L, FT4 13 pM, FT3 2.5 pM • FHx: mother, sister – both on LT4 • Medications: “Thyrosol” (health store) • Wondering about hypothyroidism causing her weight gain • Read on internet about “Wilson’s Disease”
Case 2 • When to treat “Subclinical” thyroid dysfunction? • Naturopathic thyroid remedies • Hypothryoidism Rx other than Levothyroxine • What is Wilson’s Thyroid Disease?
Subclincal Hypothyroidism • TSH, normal FT4 • Most asymptomatic & don’t need Rx (monitor TSH q2-5y) • Rx Indications: • Increased risk of progression • TSH > 10, Female > 50 y.o. • Anti-TPO Ab titre > 1:100,000 ? • Goitre present ? • Dyslipidemia? • Total cholesterol (TC) 6-8% if TSH > 10 and TC > 6.2 nM • Symptoms? • Pregnancy, Infertility, Ovulatory Dysfn.
Subclinical Hyperthyroidism • TSH, Normal FT4 and FT3 • Progression to overt hyperthyroidism low: • Men 0% per year • Women 1.5% per year • TMNG or toxic adenoma present 5% per year • Indications to Rx: • Any cardiac disease (CAD, AFIB, etc.) • Age > 60 (10 year risk AFIB 32%, 10% if normal TSH) • TMNG or toxic adenoma • Osteoporosis
Case 2 • When to treat “Subclinical” thyroid dysfunction? • Naturopathic thyroid remedies (Thyrosol) • Hypothryoidism Rx other than Levothyroxine • What is Wilson’s Thyroid Disease?
Hashimoto’s Disease • Most common cause of hypothyroidism in North America (not idodine defeciency!) • Autoimmune • lymphocytic thyroiditis • Females > Males, Runs in Families • Antithyroid antibodies: • Thyroglobulin Ab • Microsomal Ab • TSH-R Ab (block)
Hashimoto’s Disease • Treatment: • Thyroid Hormone Replacement • Levothyroxine (T4) • T3?, T4/T3 combo?, dessicated thyroid? • No benefit to giving iodine! • In fact, iodine may decrease hormone production • Wolff-Chaikoff effect (lack of escape)
Case 2 • When to treat “Subclinical” thyroid dysfunction? • Naturopathic thyroid remedies • Hypothryoidism Rx other than Levothyroxine • What is Wilson’s Thyroid Disease?
Treatment of Hypothyroidism • Iodine only if iodine deficiency is the cause • Rare in North America! • Replacement thyroid hormone medication: • T4? • T3? • T4 + T3 Mixture? • Thyroid Hormone from “natural sources” ?
Normal Daily Thyroid Secretion Rate: T4 = 100 ug/day T3 = 6 ug/day ( ratio T4:T3 = 14:1 ) T4 Protein* binding + 0.03% free T4 85% (peripheral conversion) T3 Protein* binding + 0.3% free T3 15% (10-20x less than T4)
Levothyroxine (T4) • Synthroid (Abbott), Eltroxin (GSK) • Synthetically made • 50 ug white pill no dye (hypoallergenic) • Most commonly prescribed treatment for hypothyroidism • No T3 (but 85% of T3 comes from T4 conversion) • All patients made euthyroid biochemically • Most (but not all) patients feel normal
Levothyroxine (T4) • Average dose 1.6 ug/kg • Age > 50-60 or cardiac disease: must start at a low dose (25 ug/d) • Recheck thyroid hormone levels every 4-6 weeks after a dose change • Aim for a normal TSH level
“I still don’t feel normal on Synthroid even though my blood tests are normal.” • Free T4, Free T3 • wide range of normal • TSH (0.4 –5.0 mU/L) • Narrow range of normal, but still a range! • Adjust dose for a lower TSH still in the normal range? • Tissue levels versus circulating levels? • No human studies • Rodents: High T4 and normal T3 tissue levels
Liothyronine (T3) • Cytomel (Theramed) • Shorter half-life • Fluctuating levels (i.e. need a slow-release pill) • Twice daily dosing often needed • 10x more potent: palpitations & other cardiac side effects • High T3 levels, low T4 levels (not physiologic either!)
T3/T4 Liotrix • Thyrolar • Combo pill of T3 and T4 • Ratio of T4:T3 = 4:1 (not 14:1) • T3 still not slow release • Few small studies showing benefit • 1999 NEJM study 33 patients • Benefit: mood & cognitive function • Not available in Canada
Desiccated Thyroid (Armour) • Desiccated powder derived from thyroids of slaughtered pigs or cows • Vegetarian? • Mad Cow Disease? • Contains T4 and T3 • Still no slow-release of T3 • Ratio of T4:T3 • Variable • Still not physiologic, often too high in T3 (T4:T3 = 3:1)
“In an ideal world…” • Mixed compound with T4:T3 = 14:1 • T3 component slow release formulation • Resultant: • Normal circulating TSH, FT4, FT3 • Normal tissue levels of T4 and T3 • Good, large studies (RCTs) demonstrating clear benefit over T4 alone
Case 2 • When to treat “Subclinical” thyroid dysfunction? • Naturopathic thyroid remedies • Hypothryoidism Rx other than Levothyroxine • What is Wilson’s Thyroid Disease?
“Wilson’s Syndrome” • Wilson’s disease: copper toxicity liver failure • “Wilson’s Syndrome” • Dr. E. D. Wilson “discovered” this condition and named it after himself in late 1980’s • Decreased body temperature (low normal range) • Hypothyroid symptoms (nonspecific) • Normal thyroid function tests • “Impaired T4 T3 conversion” • “Build up of reverse T3” • Treat with “Wilson’s T3-therapy” (presumably T3)
“Wilson’s Syndrome” • No scientific evidence that this condition exists • No randomized trials proving safety or any benefit of giving people T3 when their thyroid hormone levels are normal • This condition not endorsed by: • Canadain Society of Endocrinology and Metabolism (CSEM) • American Thyroid Association (ATA) • Endocrine Society
Case 4 • 29 year old female, engaged to be married • T1DM • Thyroid U/S: • 2.9 cm R lower pole • 2.0 cm L lower pole, • Many others ranging from 0.5-1.5 cm • TSH < 0.05 mU/L, FT4 19 pM, FT3 6.9 pM • RAIU/Scan: 45% RAIU, hot nodule on Left
Case 4 • FNA of 3cm nodule on Right: benign • Rx’s offered: • RAI ablation versus thyroidectomy • Patient chose Thyroidectomy
RAIU • Oral dose of I131 5 uCi (or I123 200 uCi but more $) • Measure neck counts @ 24h (+/- 4h if suspect high turnover) • RAIU = neck counts – bkgd (thigh counts) x 100 pill counts - bkgd
RAIU • Normal 4h RAIU = 5-15 % • 24h RAIU: >25% Hyperthyroid 20-25% Equivocal (check TSH) 9-20% Normal 5-9% Equivocal (check TSH) <5% Hypothyroid • Dependent on dietary iodine intake! • Must be: not pregnant! (ß-hCG), no ATD x 7d, no LT4 x 4d, no large doses of iodine or radiocontrast for 2 wk (prefer 4-6 wk)