Download
1 / 1
10 likes | 78 Views
Augmentative and Alternative Communication: The Effects of Speech Output and Iconicity on Symbol Acquisition Diana Brown, Graduate Student; Dr. Kathleen Hutchison, CCC-A, Dr. Alice Kahn, CCC-SLP; Mrs. Susan Wolfe, CCC-SLP. Influence of Cardiovascular Health on Hearing Acuity:

E N D
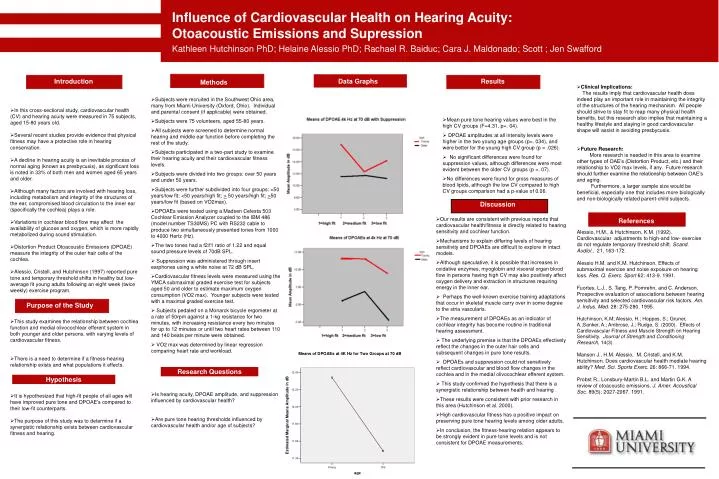
Augmentative and Alternative Communication: The Effects of Speech Output and Iconicity on Symbol Acquisition Diana Brown, Graduate Student; Dr. Kathleen Hutchison, CCC-A, Dr. Alice Kahn, CCC-SLP; Mrs. Susan Wolfe, CCC-SLP Influence of Cardiovascular Health on Hearing Acuity: Otoacoustic Emissions and Supression Kathleen Hutchinson PhD; Helaine Alessio PhD; Rachael R. Baiduc; Cara J. Maldonado; Scott ; Jen Swafford • Clinical Implications: The results imply that cardiovascular health does indeed play an important role in maintaining the integrity of the structures of the hearing mechanism. All people should strive to stay fit to reap many physical health benefits, but this research also implies that maintaining a healthy lifestyle and staying in good cardiovascular shape will assist in avoiding presbycusis. • Future Research: More research is needed in this area to examine other types of OAE’s (Distortion Product, etc.) and their relationship to VO2 max levels, if any. Future research should further examine the relationship between OAE’s and aging. Furthermore, a larger sample size would be beneficial, especially one that includes more biologically and non-biologically related parent-child subjects. • Alessio, H.M., & Hutchinson, K.M. (1992). Cardiovascular adjustments to high-and low- exercise do not regulate temporary threshold shift. Scand. Audiol., 21, 163-172. • Alessio H.M. and K.M. Hutchinson. Effects of submaximal exercise and noise exposure on hearing loss. Res. Q. Exerc. Sport 62: 413-9. 1991. • Fuortes, L.J., S. Tang, P. Pomrehn, and C. Anderson. Prospective evaluation of associations between hearing sensitivity and selected cardiovascular risk factors. Am. J. Indus. Med. 28: 275-280. 1995. • Hutchinson, K.M; Alessio, H.; Hoppes, S.; Gruner, A.;Sanker, A.; Ambrose, J.; Rudge, S. (2000). Effects of Cardiovascular Fitness and Muscle Strength on Hearing Sensitivity. Journal of Strength and Conditioning Research, 14(3). • Manson J., H.M. Alessio, M. Cristell, and K.M. Hutchinson. Does cardiovascular health mediate hearing ability? Med. Sci. Sports Exerc. 26: 866-71. 1994. • Probst R., Lonsbury-Martin B.L. and Martin G.K. A review of otoacoustic emissions. J. Amer. Acoustical Soc. 89(5): 2027-2067. 1991. • Mean pure tone hearing values were best in the high CV groups (F=4.31, p=. 04). • DPOAE amplitudes at all intensity levels were higher in the two young age groups (p=. 034), and were better for the young high CV group (p = .026). • No significant differences were found for suppression values, although differences were most evident between the older CV groups (p =. 07). • No differences were found for gross measures of blood lipids, although the low CV compared to high CV groups comparison had a p-value of 0.06. • Our results are consistent with previous reports that cardiovascular health/fitness is directly related to hearing sensitivity and cochlear function. • Mechanisms to explain differing levels of hearing sensitivity and DPOAEs are difficult to explore in intact models. • Although speculative, it is possible that increases in oxidative enzymes, myoglobin and visceral organ blood flow in persons having high CV may also positively affect oxygen delivery and extraction in structures requiring energy in the inner ear. • Perhaps the well-known exercise training adaptations that occur in skeletal muscle carry over in some degree to the stria vascularis. • The measurement of DPOAEs as an indicator of cochlear integrity has become routine in traditional hearing assessment. • The underlying premise is that the DPOAEs effectively reflect the changes in the outer hair cells and subsequent changes in pure tone results. • DPOAEs and suppression could not sensitively reflect cardiovascular and blood flow changes in the cochlea and in the medial olivocochlear efferent system. • This study confirmed the hypothesis that there is a synergistic relationship between health and hearing . • These results were consistent with prior research in this area (Hutchinson et al. 2000). • High cardiovascular fitness has a positive impact on preserving pure tone hearing levels among older adults. • In conclusion, the fitness-hearing relation appears to be strongly evident in pure tone levels and is not consistent for DPOAE measurements. • In this cross-sectional study, cardiovascular health (CV) and hearing acuity were measured in 75 subjects, aged 15-80 years old. • Several recent studies provide evidence that physical fitness may have a protective role in hearing conservation. • A decline in hearing acuity is an inevitable process of normal aging (known as presbycusis), as significant loss is noted in 33% of both men and women aged 65 years and older. • Although many factors are involved with hearing loss, including metabolism and integrity of the structures of the ear, compromised blood circulation to the inner ear (specifically the cochlea) plays a role. • Variations in cochlear blood flow may affect the availability of glucose and oxygen, which is more rapidly metabolized during sound stimulation. • Distortion Product Otoacoustic Emissions (DPOAE) measure the integrity of the outer hair cells of the cochlea. • Alessio, Cristell, and Hutchinson (1997) reported pure tone and temporary threshold shifts in healthy but low-average fit young adults following an eight week (twice weekly) exercise program. • This study examines the relationship between cochlea function and medial olivocochlear efferent system in both younger and older persons, with varying levels of cardiovascular fitness. • There is a need to determine if a fitness-hearing relationship exists and what populations it effects. • It is hypothesized that high-fit people of all ages will have improved pure tone and DPOAE’s compared to their low-fit counterparts. • The purpose of this study was to determine if a synergistic relationship exists between cardiovascular fitness and hearing. Introduction Data Graphs Results • Subjects were recruited in the Southwest Ohio area, many from Miami University (Oxford, Ohio). Individual and parental consent (if applicable) were obtained. • Subjects were 75 volunteers, aged 55-80 years. • All subjects were screened to determine normal hearing and middle ear function before completing the rest of the study. • Subjects participated in a two-part study to examine their hearing acuity and their cardiovascular fitness levels. • Subjects were divided into two groups: over 50 years and under 50 years. • Subjects were further subdivided into four groups: <50 years/low fit; <50 years/high fit; > 50 years/high fit; >50 years/low fit (based on VO2max). • DPOAEs were tested using a Madsen Celesta 503 Cochlear Emission Analyzer coupled to the IBM 486 (model number TS30MS) PC with RS232 cable to produce two simultaneously presented tones from 1000 to 4000 Hertz (Hz). • The two tones had a f2/f1 ratio of 1.22 and equal sound pressure levels of 70dB SPL. • Suppression was administered through insert earphones using a white noise at 72 dB SPL. • Cardiovascular fitness levels were measured using the YMCA submaximal graded exercise test for subjects aged 50 and older to estimate maximum oxygen consumption (VO2 max). Younger subjects were tested with a maximal graded exercise test. • Subjects pedaled on a Monarck bicycle ergometer at a rate of 50rpm against a 1-kg resistance for two minutes, with increasing resistance every two minutes for up to 12 minutes or until two heart rates between 110 and 140 beats per minute were obtained. • VO2 max was determined by linear regression comparing heart rate and workload. • Is hearing acuity, DPOAE amplitude, and suppression influenced by cardiovascular health? • Are pure tone hearing thresholds influenced by cardiovascular health and/or age of subjects? Methods Discussion References Purpose of the Study Research Questions Hypothesis






