Download
1 / 2
20 likes | 96 Views
Figure 2. Change in Frequency of Substance Use by Change in Days Exercised Group*. 0.25. 0.20. 0.15. Substance Frequency Scale (SFS). 0.10. 0.05. Time 1. Time 2. Time 3. Figure 3. Mean Days of Exercise by Exercise Group and Any Treatment. 90.

E N D
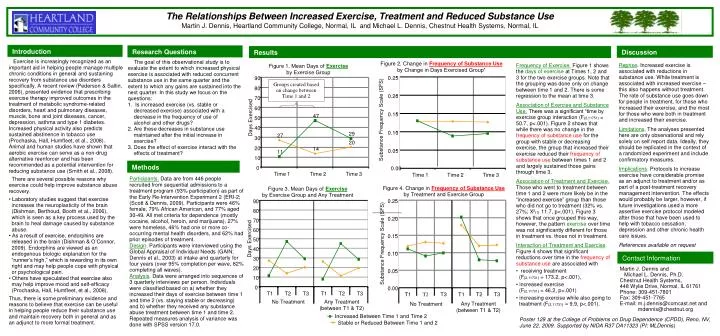
Figure 2. Change in Frequency of Substance Use by Change in Days Exercised Group* 0.25 0.20 0.15 Substance Frequency Scale (SFS) 0.10 0.05 Time 1 Time 2 Time 3 Figure 3. Mean Days of Exercise by Exercise Group and Any Treatment 90 Figure 4. Change in Frequency of Substance Use by Treatment and Exercise Group 80 0.25 70 60 0.20 Days Exercised 50 40 0.15 30 Substance Frequency Scale (SFS) 20 0.10 10 0 0.00 0.05 T1 T2 T3 T1 T2 T3 No Treatment Any Treatment (between T1 & T2) Any Treatment (between T1 & T2) No Treatment T1 T2 T3 T1 T2 T3 Increased Between Time 1 and Time 2 Stable or Reduced Between Time 1 and 2 The Relationships Between Increased Exercise, Treatment and Reduced Substance Use Martin J. Dennis, Heartland Community College, Normal, IL and Michael L. Dennis, Chestnut Health Systems, Normal, IL Introduction Research Questions Discussion Results Exercise is increasingly recognized as an important aid in helping people manage multiple chronic conditions in general and sustaining recovery from substance use disorders specifically. A recent review (Pederson & Saltin, 2006), presented evidence that prescribing exercise therapy improved outcomes in the treatment of metabolic syndrome-related disorders, heart and pulmonary diseases, muscle, bone and joint diseases, cancer, depression, asthma and type 1 diabetes. Increased physical activity also predicts sustained abstinence in tobacco use (Prochaska, Hall, Humfleet, et al., 2008). Animal and human studies have shown that aerobic exercise can serve as a non-drug alternative reenforcer and has been recommended as a potential intervention for reducing substance use (Smith et al., 2008). There are several possible reasons why exercise could help improve substance abuse recovery. • Laboratory studies suggest that exercise increases the neuroplasticity of the brain (Dishman, Berthoud, Booth et al., 2006), which is seen as a key process used by the brain to heal damage caused by substance abuse. • As a result of exercise, endorphins are released in the brain (Dishman & O’Connor, 2009). Endorphins are viewed as an endogenous biologic explanation for the “runner’s high,” which is rewarding in its own right and may help people cope with physical or psychological pain. • Others have speculated that exercise also may help improve mood and self-efficacy (Prochaska, Hall, Humfleet, et al., 2008). Thus, there is some preliminary evidence and reasons to believe that exercise can be useful in helping people reduce their substance use and maintain recovery both in general and as an adjunct to more formal treatment. • The goal of this observational study is to evaluate the extent to which increased physical exercise is associated with reduced concurrent substance use in the same quarter and the extent to which any gains are sustained into the next quarter. In this study we focus on the questions: • Is increased exercise (vs. stable or • decreased exercise) associated with a • decrease in the frequency of use of • alcohol and other drugs? • Are these decreases in substance use • maintained after the initial increase in • exercise? • Does the effect of exercise interact with the • effects of treatment? Reprise. Increased exercise is associated with reductions in substance use. While treatment is associated with increased exercise – this also happens without treatment. The rate of substance use goes down for people in treatment, for those who increased their exercise, and the most for those who were both in treatment and increased their exercise. Limitations. The analyses presented here are only observational and rely solely on self report data. Ideally, they should be replicated in the context of a randomized experiment and include confirmatory measures. Implications. Protocols to increase exercise have considerable promise as an adjunct to treatment and/or as part of a post-treatment recovery management intervention. The effects would probably be larger, however, if future investigations used a more assertive exercise protocol modeled after those that have been used to help with tobacco cessation, depression and other chronic health care issues. References available on request • Frequency of Exercise. Figure 1 shows the days of exercise at Times 1, 2 and 3 for the two exercise groups. Note that the grouping was done only on change between time 1 and 2. There is some regression to the mean at time 3. • Association of Exercise and Substance Use.There was a significant “time by exercise group interaction (F(2,11751) = 50.7, p<.001). Figure 2 shows that while there was no change in the frequency of substance use for the group with stable or decreasing exercise, the group that increased their exercise reduced their frequency of substance use between times 1 and 2 and largely sustained those gains through time 3. • Association of Treatment and Exercise. Those who went to treatment between time 1 and 2 were more likely be in the “increased exercise” group than those who did not go to treatment (32% vs. 27%; X2(1) 11.7, p<.001). Figure 3 shows that once grouped this way, however, the pattern exercise over time was not significantly different for those in treatment vs. those not in treatment. • Interaction of Treatment and Exercise. Figure 4 shows that significant reductions over time in the frequency of substance use are associated with • receiving treatment • (F(2,11731) = 173.2, p<.001), • increased exercise • (F(2,11731) = 46.2, p<.001) • increasing exercise while also going to • treatment (F(2,11731) = 9.9, p<.001). Figure 1. Mean Days of Exercise by Exercise Group 90 Groups created based on change between Time 1 and 2 80 70 60 47 Days Exercised 50 40 29 27 30 20 20 14 11 10 Methods 0 0.00 Time 1 Time 2 Time 3 Participants. Data are from 446 people recruited from sequential admissions to a treatment program (93% participation) as part of the Early Re-Intervention Experiment 2 (ERI-2; (Scott & Dennis, 2009). Participants were 46% female, 79% African American, and 77% aged 30-49. All met criteria for dependence (mostly cocaine, alcohol, heroin, and marijuana), 27% were homeless, 46% had one or more co-occurring mental health disorders, and 62% had prior episodes of treatment. Design. Participants were interviewed using the Global Appraisal of Individual Needs (GAIN; Dennis et al., 2003) at intake and quarterly for four years (over 95% completion per wave, 82% completing all waves). Analysis. Data were arranged into sequences of 3 quarterly interviews per person. Individuals were classified based on a) whether they increased their days of exercise between time 1 and time 2 (vs. staying stable or decreasing) and b) whether they received any substance abuse treatment between time 1 and time 2. Repeated measures analysis of variance was done with SPSS version 17.0. Contact Information Martin J. Dennis and Michael L. Dennis, Ph.D. Chestnut Health Systems, 448 Wylie Drive, Normal, IL 61761 Phone: 309-451-7801 Fax: 309-451-7765 E-mail: m.j.dennis@comcast.net and mdennis@chestnut.org Poster 129 at the College of Problems on Drug Dependence (CPDD), Reno, NV, June 22, 2009. Supported by NIDA R37 DA11323 (PI: MLDennis)
The Relationships between Increased Exercise, Treatment and Reduced Substance Use Martin J. Dennis (Heartland Community College) and Michael L. Dennis, Ph.D. (Chestnut Health Systems) College of Problems on Drug Dependence (CPDD) Poster 129 Reno, NV, June 22, 2009 References: Dennis, M. L., Titus, J. C., White, M., Unsicker, J., & Hodgkins, D. (2003). Global Appraisal of Individual Needs (GAIN): Administration guide for the GAIN and related measures. (Version 5 ed.). Bloomington, IL: Chestnut Health Systems. Dishman, R.K. & O’Connor, P.J. (2009). Lessons in exercise neurobiology: The case of endorphins. Mental Health and Physical Activity, 2, 4-9. Dishman, R. K., Berthoud, H., Booth, F. W., & Cotman, C. W. (2006). Neurobiology of exercise. Scandinavian Journal of Medicine & Science in Sports, 2006. Pedersen, B.K., Saltin, B. (2006). Evidence for prescribing exercise as therapy in chronic disease. Scandinavian Journal of Medicine & Science in Sports, 16 (Supplement 1), 3–63. Prochaska, J.J., Hall, S.A., Humfleet, G., Muňoz, R.F., Reus, V., Gorecki, J. & Hu, D. (2008). Physical activity as a strategy for maintaining tobacco abstinence: A randomized trial. Preventive Medicine, 47, 215–220 Scott, C. K., & Dennis, M. L. (2009). Results from two randomized clinical trials evaluating the impact of quarterly recovery management checkups with adult chronic substance users. Addiction, 104, 959-971. Smith, M.A., Schmidt, K.T., Iordanou, J.C., & Mustroph, M.L. (2008). Aerobic exercise decreases the positive-reinforcing effects of cocaine. Drug and Alcohol Dependence, 98, 129-135. Acknowledgement: Work on this poster was supported by NIDA grant R37 DA11323 (PI: MLDennis). The authors would like to thank Rod Funk, Meredith Olson, Trena Mullenix, Christy Scott, and Joan Unsicker for assistance with the study, analysis and poster. The opinions here are those of the author and do reflect official positions of the government.