Download
1 / 73
730 likes | 734 Views
Learn how to become an expert in bone density measurement in just 30 minutes. Discover the importance of treatment and how it can prevent osteoporotic fractures. Find out about different therapies and their effectiveness. Get insights into DXA reporting and improve the quality of your reports.

E N D
Becoming a worlds expert in 30 minutes • (or at least - do just as well as any world expert in 30 minutes) • No fellowship • No Big Book • The pathway has been defined and it is well paved and brightly lit.
Behold, as I guide our conversation to my narrow area of expertise
Becoming a worlds expert in 30 minutes • Bone Density Measurement BORING ! ! So - Why bother?
Disclaimer • Your presenter this morning really doesn’t care about the study. Boring. Rote. Not conceptually interesting. • Beyond that - after tax reimbursement will buy you a Venti at Starbucks
Disclaimer • But - • Your presenter really cares about not looking stupid
ME intelligent reliable worth the $ stupid unreliable not worth the $
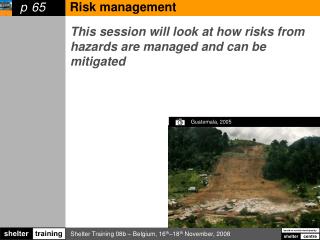
A WORD (OR MORE) ABOUT TREATMENT. WHY TREAT AT ALL??? • Osteoporotic fractures are very common in older patients, with serious sequelae • Treatment is easy, cheap and effective • OSTEOPOROTIC FRACTURES KILL PEOPLE
Osteoporotic fractures Kill 8.28 times higher risk of death for 5 years ! JAMA 2/4/2009 vol 301:5 pp 513-521
Treatment • Basic: • Adequate Calcium intake (1200 mg/day)_ • Often dietary intake adequate • Vitamin D • Exercise • Smoking Cessation • Fall prevention • Moderation in ETOH This is for everyone, regardless of density
Bone resorbtion decreased by 85% within 3 days!! MOre aggressive Treatment • Antiresorbtive therapy • Bisphosphonates • Monoclonal Antibody • denosumab • inhibits osteoclast activity and thereby reduce bone resorbtion
Treatment • Bisphosphonates: • aledronate (Binosto, Fosamax) • once per week (PO) • Generic: $10/month • zoledronic acid (Reclast, Zometa) • 5 mg every two years (IV) • Generic $994/dose = $41/month • Monoclonal ATB (esp for Renal Failure) • Denosumab: (Prolia or Xgeva) • Dosage: 60 mg SQ, every 6 months • Cost $1293 per dose ($215/month) • Particularly useful in patients with renal impairment http://health.costhelper.com/osteoporosis-treatments.html
DXA Determined by DXA + FRAX You are here When to institute therapy • Basic therapy: • All postmenopausal women • Aggressive therapy: • history of hip or vertebral fx • T-score of <-2.5 • T-score between -1 and -2.5 and • 10 year probability of hip fx > 3% OR • 10 year probability of major fx of >20% Osteoporos Int 2014; 25:2359
FRAX score helps to identify these patients Risk of fracture • Increases with decreasing bone density • T-Score <-2.5 (WHO = “osteoporotic”)most at risk • BUT: • MANY more women are “osteopenic”, therefore: • The vast majority of fractures occur in osteopenic patients • ~ 50% of hip fractures have T-score >-2.5
Effectiveness • Aldronate increases bone density Liberman UA, Weiss SR, Broll J, et al. Effect of oral alendronate on bone mineral density and the incidence of fractures in postmenopausal osteoporosis. The Alendronate Phase III Osteoporosis Treatment Study Group. N Engl J Med 1995; 333:1437.
~40% reduction in hip fractures Treatment WORKS Reduction in fracture incidence
Effectiveness • Bisphosphonates - randomized trials • reduce painful spine fractures by up to 85-90% • reduce hip fractures by 20-25% • REDUCE ALL CAUSE MORTALITY BY 28% • Despite this, most who could benefit are not treated and those who are treated < 50% continue treatment
DXA reporting:What is “right”? • International Society of Clinical Densitometry - ISCD • ISCD.org • Developed the statistical basis of the interpretation • defined what and how to report
ISCD survey • 71% of readers had seen an incorrect interpretation at least once a month • 98% of clinicians felt that poor quality reports harm patient care Lewiecki EM, et al. DXA quality matters. J Clin Densitom. 2006; 9:388–392. [PubMed: 17097522]
Report content (Key Slide)! • Density in g/cm2 (and T-score)for • fem neck • total hip • spine • (wrist) • diagnostic WHO classification • and statement on fracture risk Lewiecki EM, et al. DXA quality matters. J Clin Densitom. 2006; 9:388–392. [PubMed: 17097522]
Training animals (to include radiologists) Make the right thing easy Make the wrong thing hard
Easy reporting • What should be in the report • Templates - with modules • Module 1 - baseline or standard report • Module 2 - Comparison • Module 3 - FRAX report • Module 4 - forearm report
Module 1 - Standard report • EXAMINATION: • BONE DENSITOMETRY [<Completed Date>] • COMPARISON: • [None.] • HISTORY: • [<Reason For Exam>] • TECHNIQUE: • Bone mineral density measurements were obtained of the lumbar spine and [left hip] • Risk Factors: [Postmenopausal] • Instrument: Hologic serial number []
Module 1 -Standard report The average bone mineral density was measured across the left hip and across the spine. _____________________Density___________________T-score Left femoral neck_______ [] ________________________[] Total Left Hip___________[] ________________________[] Spine [L1-L4] __________[] ________________________[] Final categorization (based on the lowest T-score of the above, as recommended by the International Society of Clinical Densitometry): [] [] FRAX Score (likelihood of subsequent fracture) [] NOTES: 1. This facility has been validated using the recommendations of the International Society of Clinical Densitometry (ISCD). This validation insures accurate results. In order to be certain that your patient's results are accurate, you should refer them only to facilities that have been validated in this manner. Not all facilities have gone through this rigorous validation. 2. In order to compare results through the years, it is necessary that the patient be scanned on the same instrument each time, or on instruments that have been cross-correlated. If this is not done, then difference may be due to differences in the machines, rather than to changes in the patient's bone density.
The difference between these two is greater than the experimentally determined LSC for this machine, therefore, compared to prior: THERE HAS BEEN A STATISTICALLY SIGNIFICANT [] IN BONE The difference between these two is less than the experimentally determined LSC for this machine, therefore, compared to prior: NO STATISTICALLY SIGNIFICANT CHANGE Module 2 -Comparison COMPARISON WITH PRIOR EXAMINATION: Prior examination date [] Spine: Current density: [] Previous density: [] [] Left hip: Current Density: [] Previous density: [] []
The 10-year fracture risk for this patient as estimated by the FRAX tool is as follows: Major osteoporotic fracture - [] Hip fracture - [] This likelihood is based on untreated patients. No FRAX score was calculated because all T-Scores are above -1.0 (i.e. normal) The FRAX score was not calculated because the patient is in the WHO category of "osteoporotic" Module 3 -FRAX The average bone mineral density was measured across the left hip and across the spine. _____________________Density___________________T-score Left femoral neck_______ [] ________________________[] Total Left Hip___________[] ________________________[] Spine [L1-L4] __________[] ________________________[] Final categorization (based on the lowest T-score of the above, as recommended by the International Society of Clinical Densitometry): [] [] FRAX Score (likelihood of subsequent fracture) [] NOTES: 1. This facility has been validated using the recommendations of the International Society of Clinical Densitometry (ISCD). This validation insures accurate results. In order to be certain that your patient's results are accurate, you should refer them only to facilities that have been validated in this manner. Not all facilities have gone through this rigorous validation. 2. In order to compare results through the years, it is necessary that the patient be scanned on the same instrument each time, or on instruments that have been cross-correlated. If this is not done, then difference may be due to differences in the machines, rather than to changes in the patient's bone density. FRAX Score (likelihood of subsequent fracture) []
EXAMINATION: BONE DENSITOMETRY 1/20/2017 COMPARISON: 2014 HISTORY: Screening for osteoporosis TECHNIQUE: Bone mineral density measurements were obtained of the lumbar spine and left hip Risk Factors: Postmenopausal Instrument: Hologic serial number 83007 The average bone mineral density was measured across the left hip and across the spine. _____________________Density___________________T-score Left femoral neck_______ 0.556 ________________________-2.6 Total Left Hip___________0.710 ________________________-1.9 Spine L1 and L2 __________0.786 ________________________-1.8 Final categorization (based on the lowest T-score of the above, as recommended by the International Society of Clinical Densitometry): Osteoporosis L3 and L4 were excluded from the determination because of osteophytic spurs causing artifactual elevation of the density. COMPARISON WITH PRIOR EXAMINATION: Prior examination date 2014 Spine: Current density: 0.786 Previous density: 0.786 The difference between these two is less than the experimentally determined LSC for this machine, therefore, compared to prior: NO STATISTICALLY SIGNIFICANT CHANGE Left hip: Current Density: 0.710 Previous density: 0.723 The difference between these two is less than the experimentally determined LSC for this machine, therefore, compared to prior: NO STATISTICALLY SIGNIFICANT CHANGE FRAX score (likelihood of subsequent fracture): The fracture likelihood was not calculated because the patient is in the WHO category of "osteoporotic" NOTES: 1. This facility has been validated using the recommendations of the International Society of Clinical Densitometry (ISCD). This validation insures accurate results. In order to be certain that your patient's results are accurate, you should refer them only to facilities that have been validated in this manner. Not all facilities have gone through this rigorous validation. 2. In order to compare results through the years, it is necessary that the patient be scanned on the same instrument each time, or on instruments that have been cross-correlated. If this is not done, then difference may be due to differences in the machines, rather than to changes in the patient's bone density. Typical finalresult
World class in < 1 minute • Correct • Complete • Easily read
You need to know: what should be reported and what should not be reported • BUT WAIT • THERE’S MORE
What SHOULD be reported SPINE: • Report L1-L4 - EXCEPT • any vertebrae affected by “structural change”: OR have > 1.0 T - value difference from adjacent • Still - this is somewhat subjective • Must have at least 2 levels - cannot report single level • Totally fair to say the spine cannot be evaluated • in that case - add in the radius
What SHOULD be reported • Hip • Either will do • Only Total and neck, NOT Ward’s Triangle.
What SHOULD be reported Forearm: ONLY 1/3 radius value - no other is valid
What SHOULD be reported This is MOST important: Note the statistical significance of any possible change. % Change means nothing Saying “There is a statistically significant change from before” IS meaningful, and directs therapy appropriately
What Should NOT be reported • A WHO category for each level - • Only one category per patient - • lowest category of • Fem Neck, Total Hip, spine.
Following the ISCD recommendations 1) Fracture risk statement - (FRAX) Has the patient had a non-traumatic fracture ??????? Critically important, and generally, we don’t know 2) Recommendations for follow-up - best left to the clinician, I think • Difficulties
LSC • What is it? •“Least significant change” •The change in density that must be present to be 95% sure there is a “real” change. • It is a density (gm/cm2) such as 0.034. • It is not %, it is not T-score.
LSC • Can’t we use the LSC put in the machine by the company? • No • Why do they put those numbers in the report • I don’t know
LSC determination AKA: precision assessment • How do you measure it? • Each tech does 15 patients three times (three spines & three hips) • Plug results into ISCD spreadsheet. • Magically - the LSC pops out
LSC This spreadsheet downloaded from ISCD.org
BUT WAIT! • THREE EXAMS ON EACH PATIENT!!??!!! • OH - THE RADIATION!!!!
Radiation Safety • Truly - a trivial consideration http://www.radiologyinfo.org/en/info.cfm?pg=safety-xray
Radiation Safety one BED = 0.036 mSv Therefore - a patient needs to have 36 DEXA’s to = one banana http://en.wikipedia.org/wiki/Banana_equivalent_dose)
LSC determination(AKA precision assessment) Precision assessment should be standard clinical practice. Precision assessment is not research and may potentially benefit patients. It should not require approval of an institutional review board. Adherence to local radiologic safety regulations is necessary. Performance of a precision assessment requires the consent of participating patients.
LSC determination(AKA precision assessment • ISCD verbiage for patient consent: • To find out if there has been a change in your bone density, a recent bone density test is compared with a previous test. For an accurate comparison, we must know when the change is greater than the normal day-to-day fluctuation in the measurement itself. This is done by doing mathematical calculations on repeat bone density measurements of the same person made on the same day. This is called a “precision assessment.” You have been asked to participate in a precision assessment. You will have your bone density measured again at the [spine and hip] [spine, hip, and forearm]. After the first scan you will need to get off the table and then back on for the additional scan(s). The X-ray exposure involved in this is exceedingly small – typically less than the normal radiation all of us are exposed to on a daily basis. Nevertheless, you should not participate if you think you might be pregnant. Participation is up to you. If you do not wish to participate, it will have no effect on your future treatment or benefits at [clinic name].
FRAX • Fracture risk assessment tool. • EXTENSIVELY validated. • Available in most systems (for an additional charge) • Available online for free • Uses historical risk factors and neck density • Calculates % chance of fracture of spine, hip for 10 years. • Utility: Combines significant risk factors AND bone density into a single estimate which is used to determine when to treat • USING T-scores ALONE TO DECIDE TO TREAT IS ARCHAIC
FRAX • Useful for untreated patients with “low bone mass” (osteopenic) • Not valid in: • normals • Osteoporosis (T < -2.5) • “treated” patients - i.e bisphosphonates or Denusomab • Doesn’t mean Calcium
Bugaboos 1) Unusual variations of density in the spine which may or may not be explained by the images • i.e. things you run across daily that are not well defined.