Download
1 / 50
500 likes | 678 Views
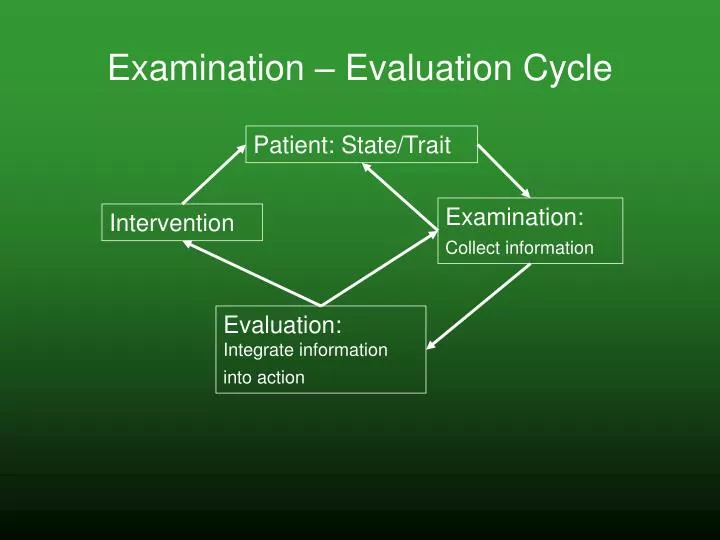
Examination – Evaluation Cycle. Patient: State/Trait . Examination: Collect information. Intervention . Evaluation: Integrate information into action. Evaluation is where you answer the question (s) that is (are) asked of you when your services are requested –

E N D
Examination – Evaluation Cycle Patient: State/Trait Examination: Collect information Intervention Evaluation: Integrate information into action
Evaluation is where you answer the question (s) that is (are) asked of you when your services are requested – • Is there an immediate need for urgent care? • Is there a need for medical referral? • Can this patient go home yet? • Can therapy Intervention help this patient? (Is there an aspect to the problem that is reversible? (May have to look at various interacting levels)) • What intervention? How long will it take? How much help? (Will save for specific interventions)
1. Is there an immediate need for urgent care? • An assessment of “stability” – if deemed not stable – needs urgent care… 2. Is there a need for medical referral? • Really is still an assessment of “stability” just on a longer time scale – if deemed stable – but at risk so needs follow up care…
3. Can this patient go home? • Again – really a question of stability on an even longer time scale • Requires an absolute yes or no answer, but is only a recommendation, so justification, pros/cons can be presented • Again – a question of “stability” over longer time frames with appropriate determination and acceptance of risks
Time scales of stability – feedback loops Coordinated & Focused Muscular Activity Work Environment Bioenergetic Process O2 Glucose H2O Ventilation CV System Respiration
What information (examination) is needed, and how to do you evaluate stability in your patient with pulmonary disease? • Urgent care… • Medical referral…. • Home……
What interventions are warranted from an evaluation that determines that a patient is not stable? • Urgent… • Medical referral…. • Home…..(see question 4)
4. Can Intervention help this patient? • Disease – Structures / Functions – Activity – Participation • What impairments seem to be causing reduced activity? How do they interact? • Are these impairments reversible? Or irreversible?
Examination – Evaluation Thought Process Cardio Pulmonary Diagnosis Yes Is the patient Stable? Examining Stability Options for intervention? No Yes Examining Endurance Impairments Does the patient have an endurance impairment? What’s the problem? No Yes Disease specific? Reversible? No Yes Interventions Interventions
Is Absolute Workload (Function) limitation associated with Reduced Endurance due toDisease Specific Impairment? Yes No • Can response be changed? • Reversible vs. Irreversible? • Medically optimized? • What does this workload allow? • Pacing • Maximize Efficiency • Conditioning • Biomechanical optimization • What is limiting factor? • Degree / time frame of reversibility? • Specific vs. General training - • Increase maximal workload • Conditioning
Functional Limitations from Endurance Impairments • Examples from ICF – limited capacity to complete the necessary workload for the required time frame when trying to… • raise up an object or taking something from one place to another, such as when lifting a cup or carrying a child from one room to another. • move along a surface on foot, step by step, so that one foot is always on the ground, such as when strolling, sauntering, walking forwards, backwards, or sideways. • carry out the coordinated actions and tasks of putting on and taking off clothes and footwear in sequence and in keeping with climatic and social conditions, such as by putting on, adjusting and removing shirts, skirts, blouses, pants, undergarments, saris, kimono, tights, hats, gloves, coats, shoes, boots, sandals and slippers. • wash and dry one's whole body, or body parts, using water and appropriate cleaning and drying materials or methods, such as bathing, showering, washing hands and feet, face and hair, and drying with a towel.
Endurance Impairments– a multi system, integrated perspective • Endurance emerges from multiple integrated systems providing energy production in a sustainable manner so that the work (task, functional activity) can be completed • Here, sustainable refers to the continuous production of energy at a sufficient level for work to continue • This has to do with where the energy for muscular contraction is coming from: • Aerobic work = sustainable for hours • Pure anaerobic work = sustainable for seconds • Balance of aerobic / anaerobic work = sustainable for up to 20 minutes, depending on the balance • At a particular workload – we all have an endurance impairment – just not resulting from disease specific reductions in system integration
Particular Impairments • Electrocardiograph Arrhythmia, Ischemia, Injury, Infarction • Chest X-Ray Pulmonary Edema Pump Effectiveness & Fluid Volume • Arterial Blood Gases Respiration • Creatinine / BUN Renal Function • Echocardiograph Pump Effectiveness (LVEF = Systolic) (EDV = Diastolic) • BNP Pump Effectiveness • Heart Sounds Pump Effectiveness • CK, Troponins Infarction • CBC Oxygen Carrying Capacity, RBC Production • Coronary Arteries (Catherization) Myocardial Oxygen Supply (MOS) • Exercise Test Oxygen Consumption / Energy Production Capacity • Respiratory Rate / Breathing Mechanics Ventilation • Lung Sounds Fluid Volume • JVD / Peripheral Edema Fluid Volume • HR x SBP = RPP Myocardial Oxygen Demand (MOD)
For all individual sources of information you need to consider: • What impairment (s) is (are) being assessed? What physiological function is assessed? Are they in isolation or aggregated with other functions? • How does this source of information relate to other sources of information? • *Why do I need this information? • Prognosis? Intervention? • *How often can I update my understanding with this information?
Capability for Work Skeletal Muscle Oxygen Consumption Oxygen Carrying Capacity Pump Effectiveness RBC Fluid Volume Systolic Diastolic Renal Function Respiration Infarction = Ventilation MOS MOD Injury < Ischemia Arrhythmia Coronary Arteries
= MOS MOD < Closer Assessment of Particular Impairments & Interactions • Coronary Arteries (Angiogram/Catherization) Myocardial Oxygen Supply (MOS) • HR x SBP = RPP Myocardial Oxygen Demand (MOD) Contributing Factors? Ischemia? Injury? Infarct? Contributing Factors? Coronary Arteries Catherization HR x SBP = RPP Contributing Factors?
Infarction = MOS MOD Injury < Ischemia Closer Assessment of Particular Impairments & Interactions • Electrocardiograph Arrhythmia, Ischemia, Injury, Infarction • CK, Troponins Infarction Pump Effectiveness Arrhythmia • Electrocardiography • ST Changes • Blocks • Biomarkers • CK; CK-MB • Troponins • Symptoms • Chest Pain / Angina • Anginal Equivalent
Biomarkers Source: Data from Christenson RH, Azzazy HME. Biochemical markers of the acute coronary syndromes. Clinical Chemistry 1998; 44: 1855-1864; Kratz, AK, Leqand – Rowski, KB: Normal reference laboratory values. New England J of Medicine 1998; 339: 1063-1072.
Infarction Injury Ischemia Closer Assessment of Particular Impairments & Interactions Echo – Cardiac Output BNP Chest XRay Heart Sounds Blood Pressure Changes Pump Effectiveness Diastolic Systolic Echo – End Diastolic Volume Echo – Left Ventricular Ejection Fraction - LVEF • Electrocardiography • Ectopic beats – PVCs, VTach, VFib • Pulse Rate • Symptoms • Palpitations Arrhythmia
Echocardiography Report Diastolic Systolic
BNP Hobbs, 2003
Chest X Ray Classic findings of congestive heart failure - note the enlarged heart, large indistinct hila, increased prominence of the pulmonary veins draining the upper lobes ("reversal of flow"), and the bilateral alveolar pulmonary edema.
Heart Sounds http://www.wilkes.med.ucla.edu/inex.htm S3: about 140-160 msec after S2, an S3 may be heard if the volume which has been transferred is abnormally large. It can be thought of as a sound which is generated when the ventricle is forced to dilate beyond its normal range because the atrium has overloaded volume. An S3 is usually heard best with the bell of the stethoscope placed at the apex while the patient is in the left lateral decubitus position. The presence of an S3 is usually normal in children and young adults, but pathologic in those over the age of 40. S4: The late stage of diastole is marked by atrial contraction, or kick, where the final 20% of the atrial output is delivered to the ventricles. If the ventricle is stiff and non-compliant, as in ventricular hypertrophy due to long-standing hypertension, the pressure wave generated as the atria contract produces an S4. It is heard best with the bell of the stethoscope at the apex.
Capability for Work Skeletal Muscle Oxygen Consumption Pump Effectiveness Systolic Diastolic Oxygen Carrying Capacity RBC Fluid Volume Renal Function Respiration Infarction Ventilation Injury Ischemia Closer Assessment of Particular Impairments & Interactions Arrhythmia
Capability for Work Skeletal Muscle Oxygen Consumption Oxygen Carrying Capacity RBC Fluid Volume Renal Function Respiration Ventilation Closer Assessment of Particular Impairments & Interactions Exercise Test CBC Chest XRay Lung Sounds Edema JVD Body Weight Creatinine BUN ABG’s RR, Breathing Mechanics
CBC / BUN / Creatinine / ABG’s • CBC – is the patient anemic? • BUN / Creatinine – are the kidneys involved? • ABG’s - is the ventilatory impairment resulting in respiratory impairment?
Exercise Test • Stress Test • Why? What? • Dobutamine Stress Test • Why? What? • Persantine Stress Test • Why? What?
Examination – Evaluation Thought Process CardioPulmonary Diagnosis Yes Is the patient Stable? Examining Stability Options for intervention? No Yes Examining Endurance Impairments Does the patient have an endurance impairment? What’s the problem? No Yes Disease specific? Reversible? No Yes Interventions Interventions
Absolute Workload (Function) Limited associated with Reduced Endurance due toDisease Specific Impairment? Yes No • Can response be changed? • Reversible vs. Irreversible? • Medically optimized? • What does this workload allow? • Pacing • Maximize Efficiency • Conditioning • Biomechanical optimization • What is limiting factor? • Degree / time frame of reversibility? • Specific vs. General training - • Increase maximal workload • Conditioning
Pulse Response Pulse with Exercise and Functional Activities • Rate • Increase with increased workload • Steady with steady workload • Recover with reduced workload • Rate Pressure Product as indicator of MVO2 • Regularity • Irregularly Irregular • Regularly Irregular
Blood Pressure Response Blood Pressure with Exercise and Functional Activities What to look for: • Drop in SBP of ≥ 10 mm Hg – modify or terminate exercise • Increase of DBP ≥ 10 mm Hg – modify or terminate exercise • Elevation of DBP when should be lower – i.e. if supine DBP is greater than standing DBP = likely failing cardiovascular system
Blood Pressure & Pulse During Breathing • Pulsus Alternans • Hold breath at midexpiration=pump failure • SBP ≥ 20 mm Hg variation • Pulsus Paradoxus • Dec. pulse strength and SBP (≥ 20 mm Hg) during inspiration • Might indicate pump failure – more likely due to COPD, cardiac tamponade, constrictive pericarditis • Deep Breathing for 1 minute at ≈ 6 bpm • Should result in decrease of HR by 15-20 bpm if not – ANS-Cardiac Dysfunction is possible
Blood Pressure & Pulse in different positions Why assess Supine vs. Standing vitals? • Status of cardiovascular regulation • If no inc HR and dec BP = ANS dysfunction • Enable perturbation of the system to determine health of the cardiovascular system • Rapid vs. sluggish (≈ 30 seconds for normal)