Download
1 / 29
401 likes | 1.27k Views
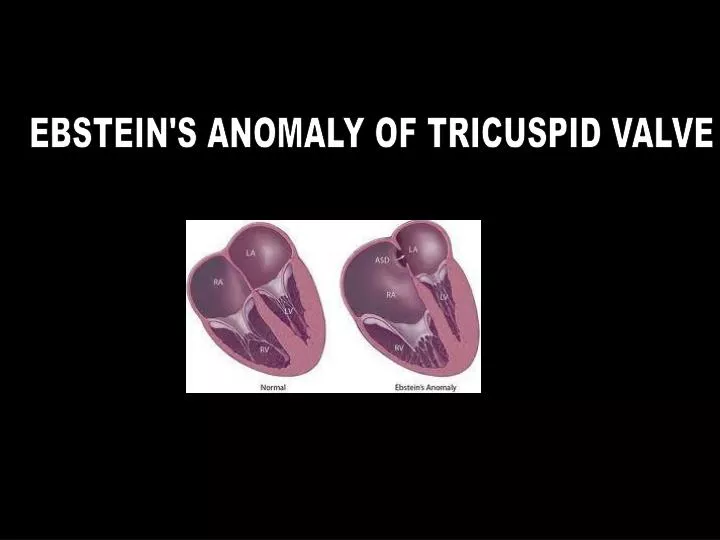
EBSTEIN'S ANOMALY OF TRICUSPID VALVE. EBSTEIN’S ANOMALY. First described by Wilhelm Ebstein in 1866 ; terminology coined by Alfred Arnstein 19 yr old cyanotic laborer with CHF at autopsy Ebstein found an enlarged and fenestrated ATL;

E N D
EBSTEIN’S ANOMALY • First described by Wilhelm Ebstein in 1866 ; terminology coined • by Alfred Arnstein • 19 yr old cyanotic laborer with CHF • at autopsy Ebstein found an enlarged and fenestrated ATL; • STL & PTL were thickened, hypoplastic and adherent to RV. • thin , dilated atrialised RV ; enlarged RA ; PFO
EBSTEIN’S ANOMALY < 1 % of CHD 1 per 200,000 live births No gender preferance Most are sporadic ; familial pattern is rare ? Genetic / reproductive / environmental risk factors • more common in twins • maternal exposure to benzodiazepines / lithium
EBSTEIN’S ANOMALY Pathology • malformation of the tricuspid valve and right ventricle • characterized by • * adherence of the septal and posterior leaflets to the underlying myocardium • (failure of delamination, namely splitting of the tissue by detachment of the • inner layer during embryologic development); • * downward (apical) displacement of the functional annulus • (septal>posterior>anterior); • * dilation of the “atrialized” portion of the right ventricle, • with various degrees of hypertrophy and thinning of the wall; • * redundancy, fenestrations, and tethering of the anterior leaflet • *dilation of the right atrioventricular junction (true tricuspid annulus)
Ebsteins Normal
EBSTEIN’S ANOMALY Pathology atrialised functional trabecular outlet Right ventricle In two third cases RV gets dilated – atrialised part RVapex RVOT
EBSTEIN’S ANOMALY Associated defects • interatrial communication in 80 - 94 % • rarely • bicuspid AV , subaortic stenosis, coarct , VSD, MVP • PS , pulmonary atresia , hypoplastic pulm. arteries Analysis of 106 cases by Jost et al (Circ.2007) Left sided anomalies in 39 % 18% of these had LV hypoplasia mimicking LV noncompaction 15 – 50 % of l – TGA has Ebstein’s like malformation of left AV valve AV bypass tracts in 20 - 30 %
EBSTEIN’S ANOMALY Classification Carpentier et al 1988 Type A - - adequate RV volume Type B - - large atrialised RV ; mobile ATL Type C - - restricted mobility of ATL > RVOT obstruction Type D - - near complete atrialisation of RV
EBSTEIN’S ANOMALY Physiology Variable – depends on the degree of pathology RV dysfunction Tricuspid regurgitation Retards forward flow During atrial systole atrialised RV balloons out acting as a passive reservoir ; during ventricular systole, much of this blood is propelled back to RA High RA pressure & low LA pressure leads to R > L shunt at atrial level
EBSTEIN’S ANOMALY Physiology Neonatal period High PVR + RV dysfunction -- behaves like pulm. atresia R > L shunt at atrial level ; ductus dependent Few weeks to months PVR falls > improvement in RV function > fall in RA pressure > cyanosis disappears Adolescence / adulthood RV failure > high RA pr . -- R > L interatrial shunt > cyanosis In patients with intact IAS .. No cyanosis; but severe CHF
EBSTEIN’S ANOMALY Clinical features Depends on the severity of malformaton Asymptomatic to severely symptomatic Cyanosis , dyspnea , palpitation , s/o CHF Cyanosis .. Typical triphasic Pulse .. Low volume ; arrhrythmias JVP .. Unimpressive Elevated ; A + / V+ Precordium .. Relatively quite despite cardiomegaly RVOT pulsation+
EBSTEIN’S ANOMALY Clinical features Auscultation Cadence of sounds • split S1 ; loud T1 ( sail sound ) • split S2 ; soft P2 • RV S3 , S4 • tricuspid OS Murmurs • TR murmur • tricuspid MDM mimics percardial rub
EBSTEIN’S ANOMALY ECG RA dilatation > tall P waves -- Himalayan P ( Taussig) Marked RA dilatation > widening & notching of P . indicates poor prognosis Right sided pre excitation in 20 – 30 % ( LAD of delta & QRS ) Without WPW RBBB pattern QRS axis .. rightward ; rarely normal / leftward polyphasic QRS in precordial leads RVH pattern .. Unusual Arrhythmias – due to RA dilatation / WPW SVT / A flutter / A fib Ventricular arhhythmias / AV blocks .. Less common
EBSTEIN’S ANOMALY Xray
EBSTEIN’S ANOMALY Echocardiogram Mmode Parasternal view .. Simultaneous visuslistion of mitral & tricuspid echoes Measure the delay from mitral to tricuspid clousre normal – 20 – 40 ms > 60 ms .. in favour of Ebsteins 2D detailed evaluation of the tricuspid valve apparatus Apical displcement of septal leaflet chambers associated lesions RV function R > L shunt at atrial level
EBSTEIN’S ANOMALY RVdilatation ; Paradoxical septal motion TV closure MV closure
EBSTEIN’S ANOMALY Echocardiogram • Apical displacement of STL • Normal .. AML to STL distance is upto 8 mm / sq. m BSA. • 15 mm / sq.m in children < 14 yrs • 20 mm /sq.m in adults Diagnostic of Ebstein’s Grading score .. Celemajor et al The ratio of the combined area of the right atrium and atrialized right ventricle is compared with that of the functional right ventricle and left heart ratio <0.5 grade 1 ratio of 0.5 to 0.99 grade 2 ratio of 1.0 to 1.49 grade 3 ratio ≥1.5 grade 4
EBSTEIN’S ANOMALY Cardaic cath Not really needed now Mainly for EPS / RFA Angiographic data can be obtained by CMR Hemodynamics Low PA and RV pressure High RA pressure Systemic desaturation Atrialised RV … RA pressure morphology with RV electrogram
EBSTEIN’S ANOMALY Management • Asymptomatic --- follow up • Newborn with cyanosis .. Maintain PDA with PGE1 • Symptomatic CHF .. Medical - digoxin , diuretics Surgery Arrhythmia .. Antiarrhtyhmics EPS > RFA Pacing for AV block ( 4 %) Cyanosis without significant TR ? Role of device closure of ASD
EBSTEIN’S ANOMALY Surgery • 1959 Repair of TV in 2 pts – both died • First successful surgery .. TV replacement • 1974 Initial publication on TVR .. 54 % mortality • Indications • NYHA III – IV • NYHA I – II + CT ratio > 0.65 • significant cyanosis • paradoxical embolism • resistant tachyarrhythmias Methods • Tricuspid valve replacement • Tricuspid valve repair .. Different techniques • one and a half ventricular repair • Heart transplant
EBSTEIN’S ANOMALY Surgery Mayo clinic series 1972 – 2005 ; 540 pts Valve reconstruction – in 35 % .. Early death – 5.4 % Valve replacement - in 65 % .. Early death - 7.6 % Technique • construction of a monocuspid valve using ATL • plication of free wall of atrialised RV • posterior tricuspid annuloplasty • reduction right atrioplasty
EBSTEIN’S ANOMALY Surgery 1988 – Carpentier et al • longitudinal plication of atrialised RV and adjacent RA • mobilisation of ATL and adjacent PTL and repositioning • to cover the orificearea at normal level • remodeling and reinforcement of annulus by prosthetic ring 191 cases early mortality 9 % mean late 20 yr survival 80%
EBSTEIN’S ANOMALY Surgery One and a half ventricular repair • tricuspid valve repair • reduction of atrialised RV • closure of ASD • end to side anastamosis of SVC to RPA
EBSTEIN’S ANOMALY Natural history Celemajor et al (JACC 1994 ) 220 cases from 1958 to 1991 ; FU 1 – 34 yrs Actuarial survival 67 % at 1 yr ; 59 % at 10 yrs Predictors of death • echo grade – 2.7 fold increase in risk • for each grade increase • fetal presentation • RVOT obstruction