Download

1 / 60
660 likes | 1.17k Views
Insulin. Refresher slides Date of preparation: June 2017 Review date: June 2018 Prepared by Donna Chorley, Pharmacist. Insulin refresher session. Types of insulin Insulin regimens Insulin errors Intravenous insulin Variable Rate Intravenous Insulin Infusion (VRIII)

E N D
Insulin Refresher slides Date of preparation: June 2017 Review date: June 2018 Prepared by Donna Chorley, Pharmacist
Insulin refresher session • Types of insulin • Insulin regimens • Insulin errors • Intravenous insulin • Variable Rate Intravenous Insulin Infusion (VRIII) • Perioperative insulin use
Types of insulin • Rapid acting analogue • Short acting (human) • Intermediate acting (human) • Long acting analogue • Biphasic mixtures (human; analogue) • Porcine and bovine rarely used
Rapid acting analogues NovoRapid (aspart) Humalog (lispro) Apidra (glulisine) ↓ risk of hypoglycaemia Short acting insulin Soluble insulin Actrapid; Humulin S; Insuman Rapid Slower onset Longer duration
Intermediate – Isophane Insulatard; Humulin I; Insuman Basal Provides background (basal) insulin (Type 2 patients) Long-acting analogues Levemir (detemir) Lantus (glargine) Tresiba (degludec) (42 hrs) Basal insulin (Type 1 & some Type 2)
Biphasic Human Humulin M3 Insuman Comb 15 Insuman Comb 25 Insuman Comb 50 Biphasic analogues NovoMix 30 Humalog Mix25 Humalog Mix50
Insulin Regimens • There is no single regimen that will suit all people • Lifestyle and eating habits need to be taken into consideration when deciding which regimen to use • Aim is to provide sufficient background (BASAL) insulin with BOLUS insulin to cover meals
Normal insulin secretion Short-lived, rapidly generated meal-related insulin peaks 70 60 50 40 Insulin (µU/ml) Low, steady, basal insulin profile 30 20 10 0 6:00 10:00 14:00 18:00 22:00 2:00 6:00 Time of day Polonsky KS et al. J Clin Invest 1988;81:442–8
Basal Bolus regimen • Allows greater flexibility • Uses rapid acting insulin just before each meal • Long acting insulin (Analogues can be given at any time but must be given same time every day) • Patients can adjust their dose according to CBG level, exercise and quantity of CHO to be eaten
Twice Daily regimen • Most common regimen used in UK • Biphasic insulin • Suitable for those with regular meal times and diet • Shorter acting component • Controls rise in glycaemic level after breakfast and evening meal • Longer acting component • Maintains glycaemic control from lunch until the early part of the evening and from late evening until the next morning • Snacks may be needed between meals and before bed to prevent hypoglycaemia
Once Daily Insulin • Type 2 only • Use of intermediate or long acting insulin • Insulatard, Humulin I • Lantus or Levemir (NICE criteria) • Needs to be given same time daily • Can be used in combination with oral antidiabetic medicines (SFU, gliptins) • Adjusted depending on pre breakfast blood glucose level
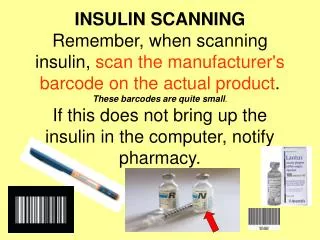
Potential errors • Omission • Insulin name / insulin type • Administration time • Insulin dose • Transfer of information • Transcription • Discharge (to GP, to community nurse) • Use of “u” or “iu” instead of units • Wrong syringe
Avoiding omission • Know who is on insulin • Always prescribe on main prescription chart as: • “Insulin – see diabetic chart” • Endorse supplementary chart section • Plan ahead: • Ensure breakfast dose for next day prescribed • If patient stable prescribe weekend doses in advance • Ensure sufficient insulin in pen/vial for next 2 doses • If insulin due after a hypo • Treat hypo • Give insulin after dose review (with meal)
Insulin Names • Use brand names • Always write name in full • Humalog Mix 25 • Humulin I • NovoMix 30 • Common errors • Humalog instead of Humalog Mix 25 • Humulin instead of Humulin I or Humulin M3 • NovoRapid instead of NovoMix 30 • Lantus / Levemir confused
Doses • Variable • Type 1 patients generally lower doses • Type 2 patients generally higher doses • Idea from King’s College Hospital • Rapid / short acting or biphasic insulin • Confirm all doses over 25 units • Intermediate / long-acting insulins • Confirm all doses over 50 units • If patients carbohydrate counting • Prescribe meal insulin as dose range e.g. 2 to 6 units • Record number of units taken
Units • Never abbreviate units • The use of “u” and “i.u” can be misread - 10 fold increase in dose given • SGUH chart pre-printed “units” • Remember to write units in full for stat doses and for dose records • Leave a space between dose and units • 22 units not 22units
Administration times • Rapid acting / (short acting) • Always for meals • Intermediate – isophane • Once or twice daily • Usually bedtime if once daily • May be given in morning • Long-acting analogues • Once or twice daily • Anytime but must be same time everyday • Biphasic mixtures • Always for meals
Insulin Syringe • Insulin syringes must be used to measure and administer insulin doses unless a pen device is used • Non-insulin syringes never used • If staff administering insulin must use safety insulin syringes
Insulin Pens and Cartridges • One pen – one patient • Store in patient’s POD locker • Stable at room temperature for 4 weeks • Discard all insulin 4 weeks after opening • Do not withdraw insulin from a pen or cartridge with a syringe • If staff administering insulin must use safety needles (Patients who self-administer should use standard insulin pen needles)
Insulin Strength • All formulary insulins at SGUH 100 units in 1ml • Be aware of higher strength insulins • Tresiba 200 units in 1ml (Flextouch pen) • Humalog 200 units in 1ml (Kwikpen) • Toujeo 300 units in 1ml (Solostar pen)
Biosimilar insulins • Not currently stocked at SGUH • Abasaglar (insulin glargine 100 units in 1ml) • Toujeo (insulin glargine 300 units in 1ml) • Be aware not directly interchangeable with Lantus insulin • Seek advice if patient admitted without own supply • Dose reduction needed for switch to Lantus
Planning for discharge • Is patient new on insulin? • Can they self administer? • Refer to Diabetes Specialist Nurse before discharge – at least 48 hours notice • Is a nurse needed to administer / monitor? • Notify community team ≥ 48 hours before discharge • Ensure insulin name, dose and times due are clear • TTO documentation • Insulin name and device • Dose at discharge and whether changed • Use duration box if necessary • Request sufficient pens for 2 weeks if supply needed
Glucose monitoring • Capillary blood glucose (CBG) • Lab sample if CBG “Hi” • How frequently? • Any specific situation? • Target range for inpatients: • 5 – 7 mmol/L (pre-meal) • Higher levels preferred for frail, older patients
Ketone monitoring • Important for patients with type 1 diabetes • Monitor for ketones • During periods of acute illness • eg infection, stress, GI disturbances • When CBG > 14 mmol/litre • During pregnancy • Presence of ketones indicates: • Need for therapy change • Possible impending / established ketoacidosis
Adjusting insulin doses • Basal bolus: • Adjust basal insulin to correct fasting glucose • Adjust bolus insulin dose for previous meal e.g. adjust breakfast insulin if pre-lunch BG high/low • Twice daily biphasic: • The breakfast injection affects the lunchtime and evening meal blood glucose • The evening injection affects the bed time level and the fasting level the next day
Insulin Titration • Adjust after several readings – review the trends • Every action has a consequence – make one adjustment at a time • Eliminate all hypoglycaemic episodes first • If need to reduce insulin dose – 10 to 20% reduction • Start the day with good glucose levels – if CBG high throughout day normalise fasting level first • If need to increase insulin dose - 10% increment • DON’T prescribe prn insulin
Insulin titration cont’d • PRIOR to adjusting DON’T forget to check: • Injections Sites – where is the insulin being injected? • What is the patient eating or drinking? • Has any new medication been initiated that could have affected the glucose levels? • Has the right insulin been prescribed?
Prescription review • Review the type of insulins patient is taking • Why is patient on basal insulin and a biphasic? • Why is the patient taking biphasic insulin and gliclazide? • Are the administration times correct? • Rapid/short and biphasic never given at bedtime
Intravenous insulin – Indications • NBM (variable rate) • Peri-operative / Peri-procedure (variable rate) • DKA / HHS (fixed rate) • Patients who are vomiting (variable rate) • Patients with hyperglycaemia complicating acute renal, cardiac or liver failure (variable rate) • Treatment of hyperkalaemia (fixed rate)
Risks / Benefits • Advantages of VRIII • Flexibility for independent adjustment of fluid and insulin • Accurate delivery of insulin via syringe driver • Allows tight BG control in the intra-operative starvation period • Disadvantages of VRIII • Risk of adverse events leading to serious incidents • Reactive to BG levels not proactive • Increased staff time for monitoring • Delays and difficulties in transfer back to normal regimen may prolong length of stay
Insulin infusion rate • Rate determined by: • Insulin sensitivity • Type 1 patient on low dose subcutaneous insulin dose is sensitive to insulin and requires lower rate • Type 2 patient on large subcutaneous insulin doses is insulin resistant and requires higher rate • Whether long-acting insulin given in previous 12 hours • If Lantus or Levemir given basal requirements met and can infuse at lower rate with a zero option • If no basal insulin given need continuous infusion
Oral anti-diabetic agents but no s/c insulin – initial scale 1 or 2
Fluid management with iv insulin • Provide glucose as substrate (fuel) to prevent proteolysis, lipolysis and ketogenesis • Optimise intravascular volume status • Maintain serum electrolytes within normal ranges • Current recommendations • 0.45% NaCl + 5% glucose + 0.15% KCl • 0.45% NaCl + 5% glucose + 0.3% KCl
Monitoring • Capillary Blood Glucose (CBG) • Every hour • If out of range increase frequency • Potassium • Ideally every 4 hours (VRIII) • In practice if in range 2 readings in 24 hours acceptable • Sodium • Ideally every 4 hours (VRIII) • Cannula and infusion devices • Duration • Refer to diabetes team if duration > 24 hours
Monitoring blood glucose • Monitor CBG every hour • Aim for CBG range 6 to 10 mmol/L • If hyperglycaemia • CBG >12 mmol/L for 3 readings and not falling by ≥ 3mmol/L per hour • Ensure infusion devices and cannula patent • Prescriber to increase to next scale • If hypoglycaemia (CBG < 4mmol/L) • Reduce rate to 0.5 units/hour • If scale zero stop infusion until hypoglycaemia treated • Treat hypoglycaemia • Adjust scale once CBG > 4mmol/L
Successful IV Insulin Infusion Mmol/l 10 6 Desired Pattern Desired Pattern Undesirable Pattern
Hypoglycaemia • Most common side effect of iv insulin • Prevent by frequent CBG monitoring • Treat for “hypo avoidance” • Adjust insulin dose • 100 ml 10% glucose iv prn prescription
Stopping iv insulin • Patient eating and drinking; not vomiting • Intravenous insulin • Half life 3 to 5 minutes • Duration 20 to 30 minutes • First dose of subcutaneous insulin must be given 60 minutes before stopping iv • If basal insulin (Levemir, Lantus, Tresiba) continued alongside VRIII can stop VRIII at any time