Download
1 / 47
470 likes | 487 Views
Percutaneous Vertebroplasty and Vertebral Augmentation. for treatment of Vertebral Compression Fractures. Pathology of VCF. Facts on Osteoporosis. It is estimated that 10 million Americans have established osteoporosis and another 34 million have osteopenia, or low bone

E N D
Percutaneous Vertebroplasty and Vertebral Augmentation for treatment of Vertebral Compression Fractures
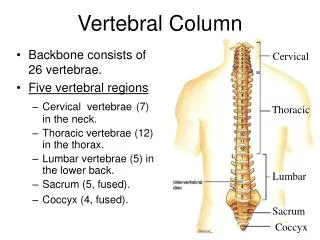
Facts on Osteoporosis It is estimated that 10 million Americans have established osteoporosis and another 34 million have osteopenia, or low bone mass, which leads to osteoporosis. Osteoporosis is responsible for 1.5 millions fractures annually, mostly involving the lumbar vertebrae, hip, and wrist. About 80% of women and 20% of men are expected to have osteoporosis in their lifetime. The estimated cost for osteoporosis and associated fractures is $13.8 billion a year (Iqbal 2000). For women between the ages of 65 and 84 years, 85% of hip and spine fractures are attributable to osteoporosis. Over 700,000 people are diagnosed with vertebral compression fractures (VCFs) each year but only a small percentage are treated.
Pathology of VCFs After menopause, there is a rapid loss of cancellous bone, removing some of the trabecular structural elements of the bone Bone loss continues after the initial post-menopausal stage, further reducing bone structure. Normal bone Patients with VCFs are found to have fewer trabecular elements, rather than global thinning of trabeculae VCFs are sustained when minimal force is applied to weakened bone structure. Osteoporotic bone
Clinical Consequences of VCFs Of clinically detected fractures, 84% are associated with pain Timing is key to treat success (NEJM, 2009) The greater the deformity of the fracture, the greater the pain and disability: – Reduced exercise tolerance – Early satiety and weight loss – Functional decline, reduced ability to perform ADLs – Depression, loss of self-esteem, sleep disorders – Kyphotic deformity resulting in gastrointestinal and pulmonary dysfunction. – Increased hospitalization and mortality
Traditional therapy for VCFs • Preventative: – Hormone replacement therapy – Biphosphonates – Calcitonin • Symptomatic relief: – Analgesics – temporary, side effects – Bed rest – risk of deep venous thrombosis – Immobilization/bracing – Surgery (rare) • Limited success of traditional therapies – Many patients report intractable pain without narcotics – Inability to return to normal activities
It’s Your Responsibility!!! The patient failed conservative care by nature of FX Treating osteoporosis is more than kypho. Forteo>Prolia>Bisphosphonates>Ca+D http://courses.washington.edu/bonephys/opPTH.html Forteo must be first line as preserving existing bone is not good enough, they already fractured. Canadian Guidelines: Forteo 1stline AACE 2010 Grade A Best level evidence for high risk
Effect of PMMA on VCFs • Main benefit of vertebroplasty: pain relief • While the precise mechanism of pain relief has not been proven it is believed to be achieved by: – Immobilization of the fracture – Relieving stress on the remaining bone by providing increased tensile strength and stiffness – Destruction of nerve endings by causing necrosis through: • Heat – exothermic reaction of monomer and polymer in the cement • Direct toxic effect
VCF Classifications Retropulsion
Options • Medical tx ltd to – Pain control, Bracing, Bedrest • Surgery often contraindicated – Too soft to hold instrumentation • Inactivity may cause (1-4): – PE/Pneumonia/Bone & Muscle loss • PMMA injection – Stabilizes fx – ↓ pain & ↑ ambulation5
Treatement Options – Noninvasive Mgmt “Conservative Care?” Opiate side effects12 ↑ Kyphosis8 ↓ Pulmonary fxn8,7 Depression12 ↓ Quality of life13 ↑ Mortality9
Indications for Vertebroplasty Painful osteoporotic fractures less than one year old Pain refractory to traditional medical therapy – No long-term relief with analgesics (and/or side effects to dosage includes excessive drowsiness, confusion or constipation) – Pain negatively impacting mobility and ADLs – Worsens with weight bearing – Relieved with rest or when recumbent Painful fracture related to benign or malignant tumor (metastatic disease, hemangiomas) Patient with multiple compression fractures for whom further collapse would result in compromised pulmonary or GI function
Indications for Vertebral Augmentation Unstable compression fracture with movement at the wedge deformity Chronic traumatic fracture with non-union of the fracture fragments Pain from fracture localized to site of the fracture (or 1-2 levels away) – tender on palpation Often band-like radiation of pain Radiographic evidence of compression fracture Negative CT/MRI for HNP, retropulsed fragment Unstable wedge fracture
LCD: GA The performance of Vertebral Augmentation Procedures (VAPs) are considered to be medically reasonable and necessary in the following conditions: Persistent debilitating pain caused by the recent (e.g. 8 – 12 weeks) pathologic fracture or collapse of noncervical vertebrae. – Initially, conservative management should be implemented prior to performing a VAP. Conservative management includes, but is not limited to, immobilization, analgesia, physical therapy, etc. – Exceptions to conservative management may include a high level of pain, disability and neurologic compromise. •Painful non-unions of Vertebral Compression Fractures (VCF) •Back pain associated with osteolytic metastatic disease involving a vertebral body •Back pain associated with multiple myeloma involving a vertebral body •Painful hemangiomas. Limitations Coverage for only one procedure per lifetime per vertebra will be allowed. If a repeat procedure on a single vertebra is to be performed, medical record documentation must support the medical necessity of the repeat procedure. •Medicare will not provide coverage for procedures performed for asymptomatic VCFs, VCFs responding appropriately to conservative therapy, or for healed VCFs. •Bone biopsy is considered integral to the procedures and not separately billable. •Treatment of kyphosis in the absence of a painful VCF is not covered. •VAPs is contraindicated in osteomyelitis / discitis involving the vertebral column.
Doo, Shin, et al J Korean Med Sci 2008 23:1005-10
Patient Selection When do you offer intervention?
Parapedicular Approach
Lobel: Start to finish 1. Review MRI with STIR, pick approach 2. Get patient in good position for both them and you 3. Scout fluoro from T6 to sacrum, match fractures 4. Using MRI knowledge, pick trajectory 5. Wide prep, wide drape, lots of local 6. Get needle perfect. Finish where you start!!! 7. Pull back, balloon, cement, 360, no straws.
Thank you. All slides and data are available for you. Questions appreciated. lobelsteve@gmail.com
Transpedicular Approach - Troubleshooting • Trajectory too flat • Final placement will be posterior & contralateral Slide Courtesy of Douglas P. Beall, M.D.
Transpedicular Approach - Troubleshooting Trajectory too steep Final placement will be anterior and on near side
Fracture Age and Ability to Reduce 35% Loss of Height 75% Loss of Height Nov 28, 2004 Feb 23, 2005 – Many fractures progressively collapse – Reduction is more predictable when fracture is acute
Indications Painful VCF’s due to osteoporosis, trauma or tumor Inadequate pain relief w/ analgesics, bracing & activity modification Contraindications: • Uncorrected coagulopathy • Infection • Allergy to any required component • No pain
Pre-Procedure Imaging X-rays • Compare w/ prior studies! • Evaluate height loss • Look for retropulsion Bone Scan • Preferably w/ SPECT (to assess post. elements/facet jt) • R/O metastatic disease • Use CT & Bone Scan when MRI can’t be used
Pre-Procedure Imaging • MRI –T1, T2, STIR sequences –Assess for marrow edema –Exclude critical stenosis –Assess cortical integrity • CT –If MRI is contraindicated –Excellent bone detail i.e. Eval post cortical wall
Pre-procedure Evaluation • ID Correct Level –Via Data from Imaging & Phys Exam –Symptomatic levels may not be compressed & • Compressed levels may not be symptomatic
Needle Positioning & Placement Accurate needle placement is critical for effective cement injection and to reduce risk of complication Use of high-quality fluoroscopy imaging equipment is critical to get accurate needle placement Transpedicular approach is safest; often bilaterally 11 G needle for lumbar and lower thoracic spine; 13 gauge for mid to upper thoracic
Needle Positioning Transpedicular Parapedicular
With A-P & Lateral views, anywhere in “the box” appears in the vertebral body Slide Courtesy of Douglas P. Beall, M.D.
Needle Tip Placement Too Far Anterior Slide Courtesy of Douglas P. Beall, M.D.
Anatomic Landmarks • Pedicles – To define starting point of trocar (the safe triangle) – In upper half of VB on AP view • Spinous Process – Indicates AP or degree of obliquity • Endplates – Defines AP view & needle trajectory post to ant (parallel)
True A-P Image & Lateral Images Pedicles upper ½ of VB Endplates parallel Pedicles & ribs superimposed Spinous process in midline
ANATOMY-SCOTTY DOG Lumbar Thoracic P=pedicle arrows=medial pedicle