Download

1 / 32
320 likes | 321 Views
This study explores the role of recurrent glomerular diseases in kidney transplantation and the use of protocol biopsies in improving our understanding of these diseases. It also examines the causes of graft loss and the importance of early diagnosis and treatment.

E N D
Role of recurrent disease for late allograft loss Fernando G. Cosio Mayo Clinic, Rochester MN 10th Banff conference on allograft pathology
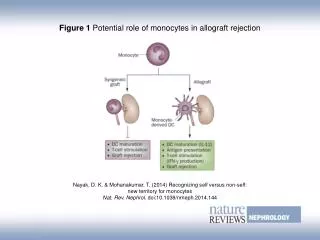
Issues to be addressed • Relevance of recurrent disease to the overall outcomes of kidney transplantation. • Role of protocol biopsies in improving our understanding of recurrent glomerular diseases. • Role of protocol biopsies in improving our understanding of glomerulonephritis
Causes of Graft Loss in 1317 conventional recipients transplanted between 1996-2006 F/u months: 50 ± 33 (0-138) (Ziad El-Zoghby, Cosio AJT 9:527-535, 2009)
Mechanisms of death-censored kidney graft loss (1996-2006) 1317 transplants 153 losses Antibody-mediated Cell-mediated (Ziad El-Zoghby, Cosio et al AJT 9:527-535, 2009)
Recurrent non-glomerular diseases • Graft losses due to recurrent non-GN disease: 7/153 (5%) • Oxalosis 2 • Sickle cell anemia 1 • Light chain DD 1 • HUS/TTP 1 • Scleroderma 2
Causes of renal failure in transplant recipients: Mayo versus USA
Mayo Clinic experience with recurrent GN: Preliminary analyses • 1317 kidney recipients transplanted from 1996-2006. • Subpopulations: • Controls: 172 patients with ADPKD • Patients with GN (FSGS, MN, MPGN) • End points: • Death-censored graft survival • Disease recurrence (protocol Bx) • General observations (vignettes)
Kidney transplantation in focal segmental glomerulosclerosis (FSGS) • Compared to PKD, recipients with FSGS have reduced death-censored graft survival. • Only patients with FSGS and recurrence have reduced graft survival. PKD, N=172 FSGS - recurrence PKD 71% FSGS, N=103 58% FSGS + recurrence p=0.0048 p<0.0001
Kidney transplantation in FSGS Present with higher grade proteinuria but no FSGS lesions • 103 patients with FSGS (unselected) (8% of recipients) • 35% recurrence (clinical and/or histologic) • Median time to recurrence: 6.9 months (0.01-116) Often subclinical with minor proteinuria and FSGS on protocol bx 41% 44% 16%
Kidney transplantation in membranoproliferative GN (MPGN) • 25 patients with MPGN (excluding type II, fibrillary and secondary forms). • 2% of recipients. • Reduced graft survival compared to PKD. • 17% of grafts lost due to recurrence PKD (N=172) MPGN (N=25) p=0.048
Kidney transplantation in MPGN • 41% recurrence at 3.7 months (0.36-17.9) post-Tx. • Higher likelihood of recurrence: • Low C3 or C4 • Living donors • Monoclonal proteins Low C3 and /or C4 Nl C3 and C4 p=0.020
Kidney transplantation in membranous nephropathy (MN) • 31 patients with MN. • 2% of recipients. • 42% recurrence at 2.5 months (4-64) • Histologic recurrence is often subclinical for several months • 11% of grafts lost due to recurrent MN PKD (N=172) MN (N=31) p=0.284
Protocol biopsies and recurrent disease: Postulates • Protocol biopsies may allow early diagnosis of recurrent GN before it is clinically apparent. • The earliest histologic changes of GN may give us clues about the pathogenesis of these diseases. • Early histologic diagnosis may allow more effective treatment.
Course and management of GNs in native kidneys: current status Progressive disease justifies treatment Disease starts Clinical diagnosis Histologic diagnosis ? • Waiting period due to the following issues: • Disease may go away? • Treatments are toxic and partially effective • Deployment of appropriate treatment is difficult
Protocol biopsies suggest several interesting questions / possibilities Progressive disease justifies treatment Disease starts Clinical diagnosis Histologic diagnosis How do these diseases look like when they start? • Does the histologic Dx precede clinical manifestations? • Are there variables that relate to this transition? Should we treat based on histology? Can we thus achieve better results? Improve kidney prognosis?
A familiar challenge: diagnosis of recurrent FSGS without FSGS 4 month protocol Bx. Urine protein 420 mg/day. EM: focal FPF Original Dx: FSGS 5 month clinical Bx. Urine protein 6030 mg/day. LM: normal. EM: diffuse FPF 12 month protocol Bx. Urine protein 1030 mg/day. LM: FSGS, finally!
Diagnostic challenges are also pathogenic lessons • 51 yo recipient of a kidney transplant in 1/2008. Original disease MN. • One month post-Tx surgery is done for lymphocele (creatinine). A biopsy done during Sx. Urine protein 179 mg/day. • Light microscopy: Normal, no “spikes” no deposits. C4d done…
C4d C3 IgG
Protocol biopsies and diagnosis of recurrent GN • Protocol biopsies can make pre-clinical diagnoses of some GN. • Current diagnostic criteria for GN are invalid: • FSGS without F, S, G or S • MN without C3 or EM deposits • MPGN without MP
Next question: Does a pre-clinical diagnosis lead to clinical disease? • 19 patients with MN diagnosed by protocol biopsy and followed, untreated for at least one year: • 2 (10.5%) have maintained low levels of proteinuria. • 17 (89.5%) have had progressive proteinuria • Repeat biopsies: MN in all (no spontaneous histologic remissions)
Protocol biopsies early diagnosis or over-diagnosis? Tx year: ‘00-’07 Dx: protocol Bx (N=30) Recurrence: 42% Median months to recurrence: 4 (2-61) Tx year: ‘90-’99 Dx: clinical with Bx confirmation (N=20) Recurrrence: 55% Median months to recurrence: 83 (6-149)
Postulated benefits of protocol biopsies in recurrent GN • Early, pre-clinical diagnosis • Pathogenic clues • Early histologic diagnosis may allow more effective treatment (preliminary studies suggest that we can/should start to explore this question)
Interesting initial observations treating recurrent MN 1y after Rituximab (no proteinuria) • Rituximab treatment of recurrent MN: • (1y) 75% complete or partial clinical remission • (2y) Evidence of DD resorption in 6/7 • (2y) Negative IgG (4/7) and negative C3 (3/7) Diagnosis(4 mo post-Tx) 2 y after Rituximab (no proteinuria)
45 yo female with SLE. LRD kidney transplant 2/2007… • What do we do now? • Current approach: do not treat unless the disease is clinically apparent… • Should we explore alternative approaches?
Recurrent disease • 20% of death-censored graft losses are due to recurrent disease (15% rGN). • Studies using protocol biopsies suggest: • Need diagnostic criteria for early dis. • Need multicenter studies based on protocol biopsies to determine: • Histologic diagnosis clinical? • Effectiveness early Rx? • We finally have good questions and reasonable tools to try to answer them!
If we knew what we were doing it would not be called research A. Einstein Recurrent disease after kidney transplantation-- it is time to unite to address this problem! A. Matas
If we knew what we were doing it would not be called researchA. Einstein In addition,
Graft loss by cause in 1317 transplants recipients (1996 to 2006) Graft failure Death (Ziad El-Zoghby, Cosio AJT 9:527-535, 2009)
Impact of recurrent glomerular diseases on death-censored graft survival (Ziad El-Zoghby, Cosio AJT 9:527-535, 2009)