Download
1 / 25
250 likes | 333 Views
EARLY ACS Trial Rationale and Design. Robert A. Harrington, MD, FACC, FSCAI Professor of Medicine Duke Clinical Research Institute Duke University Medical Center. NSTE Acute Coronary Syndromes: Key Issues 2005. High-risk NSTE ACS patients

E N D
EARLY ACSTrial Rationale and Design Robert A. Harrington, MD, FACC, FSCAI Professor of Medicine Duke Clinical Research Institute Duke University Medical Center
NSTE Acute Coronary Syndromes:Key Issues 2005 • High-risk NSTE ACS patients • multiple medical therapies; invasive strategy of care • high event rates • Platelet GP IIb/IIIa inhibitors • Broad populations versus targeted high-risk • Timing of initiation: “upstream” versus PCI; CABG • Data in contemporary practice (concomitant therapies) • Clopidogrel • Timing of initiation • Bleeding risk in CABG
And… • The Unabomber is sentenced. • Clinton testifies before a grand jury. • The Backstreet Boys make it big.
1.0 0.95 Freedom from Death / MI 0.9 0.85 Enoxaparin UFH 0.8 0 5 10 15 20 25 30 Days from Randomization Death or MI at 30 Days 1.1 HR 0.96 (0.86-1.06)
Concomitant Medications Enoxaparin UFH (n = 4993) (n = 4985) Aspirin (%) 95 95 Beta blocker (%) 86 86 Ace inhibitor (%) 64 62 Statin (%) 69 70 Clopidogrel (%) 62 63 GP IIb-IIIa inhibitor (%) 56 58
PARAGON B PRISM CAPTURE COMBINED 0.125 0.125 0.125 1 2 1 2 1 2 TnT-negative TnT-positive Interaction “Protein-Targeted” Treatment Strategies in ACS:Benefit of GPIIb/IIIa Inhibitor by Troponin Status -Newby LK, et al. Circ 103:2891;2001
GP IIb/IIIa Blockade Before and After PCI: CAPTURE, PURSUIT, PRISM-PLUS Before PCI Post-PCI 10% Placebo GP IIb/IIIa inhibitor 8.0% 8% 6% N=12,296 P=0.001 Death or MI 4.9% 4.3% 4% 2.9% N=2754 P=0.001 2% 0% +24 h +48 h +72 h +24 h +48 h 0 PCI -Boersma E, et al. Circulation, 1999
Abciximab vs. Placebo in PCI after pretreatment with Clopidogrel (ISAR-REACT) Kastrati et al. N Eng J Med 2004
Clopidogrel: Balancing Efficacy and SafetyUncertainties Regarding Timing of Therapy Early treatment • Reduced early ischemic events • Potential for bleeding if early CABG needed Wait until catheterization • Avoid treatment of patients pre-CABG • Lost opportunity for early benefit
ACC/AHA 2002 Guideline Update for the Management of Patients with UA and NSTE MI Class I A platelet GP IIb/IIIa antagonist, should be administered, in addition to aspirin and heparin, to patients in whom catheterization and PCI are planned. The GP IIb/IIIa antagonist may also be administered just prior to PCI. (Level of Evidence: A) Class IIa A platelet GP IIb/IIIa antagonist should be administered to patients already receiving heparin, aspirin, and clopidogrel in whom catheterization and PCI are planned. The GP IIb/IIIa antagonist may also be administered just prior to PCI. (Level of Evidence: B)
50% 40% 40% 40% 36% 30% 20% 20% 10% 0% GP IIb/IIIa Clopidogrel GP IIb/IIIa + Neither Clopidogrel Acute (< 24 hrs) Anti-Platelet Therapies High-Risk NSTE ACS in CRUSADE CRUSADE Q2 2003 data
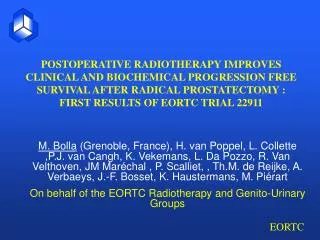
Early Glycoprotein IIb/IIIa Inhibition in Non-ST-segment Elevation Acute Coronary Syndrome: A Randomized, Double-blind, Placebo-Controlled Trial Evaluating the Clinical Benefits of Early Front-loaded Eptifibatide in the Treatment of Patients with Non-ST-segment Elevation Acute Coronary Syndromes
Trial Organization Millennium • Sponsor Schering-Plough (SPRI) • Sponsor • European Site Management • Drug Distribution for sites outside North America International Steering Committee • Scientific & Clinical Leadership DCRI/ CVC • Scientific & Clinical Leadership • North American Site Management • Coordinating Center • Data Management TIMI • Scientific & Clinical Leadership International Steering Committee Schering- Plough Millennium Partnerships Sites Patients ICTI/ IVRS DCRI/ CVC CTS Durham Pharmacy TIMI
Primary Objective To demonstrate the superiority of early eptifibatide compared to placebo (with provisional use of eptifibatide in the cath lab) in reducing the composite of death, MI, recurrent ischemia, and thrombotic bail-out within 96 hours in patients with high-risk NSTE ACS managed with an early invasive strategy
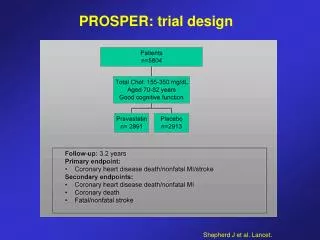
Study Design • 2 of 3 criteria: • Age > 60 yo • + CKMB or TNT/I • ST or transient ST High-risk NSTE ACS n = 10,500 Eptifibatide (180/2/180) Placebo Randomize within 8 hours Early invasive strategy: no sooner than next calendar day 1 Endpoint: 96-hr Death/MI/Urgent Revasc/Thrombotic bailout 2 Endpoint: 30 d Death/MI
Concomitant Therapies • Aspirin • Enoxaparin or Unfractionated Heparin • Dosing guides provided in protocol • Lessons from SYNERGY • Use of bivalirudin or other direct thrombin inhibitor is prohibited • Clopidogrel 300 mg load / 75 mg daily dose • Randomization stratified by investigator’s intention to start clopidogrel pre-cath
Blinded Study Drug Administration • Duration of infusion • Medically managed • Minimum = 72 hours; maximum = 96 hours • Percutaneous coronary intervention • Minimum = 72 hours; maximum of 96 hours • Continue for 18 hours after procedure • Coronary Artery Bypass Surgery • Maximum of 120 hours • Continue infusion until 2 hours before surgery
Use of Eptifibatide in the Cath Lab(1) After Angiography and Before PCI • Eptifibatide during PCI according to local practice • PCI active treatment kits are available for use after the diagnostic angiogram and before PCI begins • Kit contents are opposite of the initial study drug assignment at randomization • PCI active kits are used for the bolus doses of eptifibatide/placebo (no charge), open label hospital supply of eptifibatide is used for the infusion • Use of PCI active kits before PCI begins is not considered a study endpoint
Use of Eptifibatide in the Cath Lab(2) After PCI Has Begun • Once the guidewire crosses the lesion, use of bail-out study drug is permitted to manage complications of PCI, but is considered an endpoint event • Decrement in TIMI flow grade or abrupt closure • Dissection with decreased flow • Distal embolization • Side-branch closure • Clinical instability due to ischemia or prolonged ischemia during the procedure
Study Endpoints • Primary Efficacy Composite (96 hours) • All cause mortality • New MI*, • Recurrent ischemia requiring urgent revascularization*, • Need for thrombotic bailout with GP IIb/IIIa* • Key Secondary Efficacy Endpoint • Death or new MI* through 30 days • Safety Endpoints • Hemorrhage, transfusion, stroke*, thrombocytopenia, SAEs, post-operative bleeding *Adjudicated by independent, blinded CEC
Statistical Methods • Power = 85% to detect a 22.5% reduction in the primary quadruple composite assuming an event rate of 5.8% with placebo • Power = 85% for the key secondary efficacy endpoint of death or MI at 30 days (15% RRR, placebo rate 12.7%) • Prespecified subgroups • Proper: Age, baseline troponin, hospital type, diabetes, early clopidogrel, UFH vs enoxaparin, TIMI Risk Score • Improper: By management strategy (PCI, CABG, medical)
Local hospital lab: WBC, creat, FBS, Hgb A1C Core Lab (NA only): inflammation, ischemia, necrosis, hemodynamic stress, thrombosis 3 timepoints: baseline, pre-cath, 1 day post-cath DNA specimen: (NA only) at baseline Objectives Identify high-risk NTE-ACS patients Explore the ability of eptifibatide to modulate cardiac biomarkers Identify patients who benefit most from early eptifibatide Biomarker Substudy
Platelet Inhibition in NSTE ACSSummary of Current Status • NSTE ACS remains major clinical challenge • Equipoise around best timing of initiation of GP IIb/IIIa inhibitors in high-risk NSTE-ACS patients in whom invasive strategy planned • Uncertainties about the use of clopidogrel in high-risk NSTE-ACS in whom invasive strategy planned • Optimal combination of antithrombotic Rx is uncertain