Download
1 / 106
1.1k likes | 1.41k Views
Carpal Tunnel Release - Open . Neuro Procedures Operative Sequence. Carpal Tunnel Release - Open. Overall Purpose of Procedure : Carpal Tunnel release is performed to eliminate or significantly decrease the pressure on the carpal canal and the median nerve. Carpal Tunnel Release - Open.

E N D
Carpal Tunnel Release - Open Neuro ProceduresOperative Sequence
Carpal Tunnel Release - Open Overall Purpose of Procedure: Carpal Tunnel release is performed to eliminate or significantly decrease the pressure on the carpal canal and the median nerve.
Carpal Tunnel Release - Open Define the procedure: Cutting of the Transverse Carpal Ligament to relieve tension in the canal.
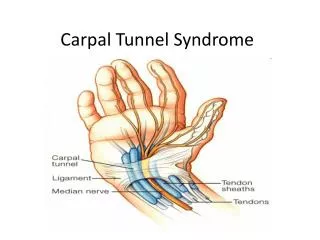
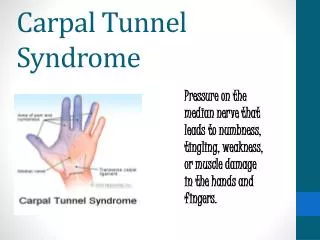
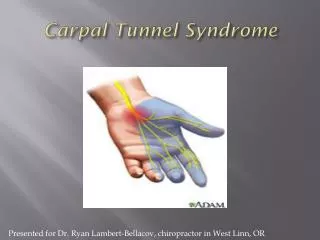
Carpal Tunnel Release - Open • Any condition that decreases the size of the canal may cause pressure on the median nerve with resultant symptoms of carpal tunnel syndrome. This manifests as pain and parathesia in the thumb, the index finger and the radial half of the ring finger. • Conditions which contribute to the compression of the medial nerve include (but are not limited to): • - fracture of a carpal bone, hypertrophic synovitis of RA, tumors, ganglion, lipomas, systemic conditions such as: • Obesity, diabetes melitis, thyroid dysfunction, and Raynaud's disease (is a vascular disorder that affects blood flow to the extremities) and pregnancy. • This syndrome occurs more often in women.
Carpal Tunnel Release - Open Wound Classification: 1
Operative Sequence 1- Incision 2- Hemostasis 3- Dissection 4- Exposure 5- Procedure (Specimen Collection possible) 6- Hemostasis 7- Irrigation 8- Closure 9- Dressing Application
Carpal Tunnel Release - Open Instrumentation: Minor Ortho tray or Hand Tray. Positioning: Supine with arms on arm boards. Affected arm on Hand Table Prepping: Surgeon preference. Duraprep, Hibiclense or a Betadine Prep Kit. Draping: Towel around tourniquet. Hand Table Drape. Possible Stockinette and Coban.
Carpal Tunnel Release - OpenBegin your Operative Sequence Prior to Incision: hair on patients arm is not usually removed. Place arm on bump for circumferential prep. Incision: Skin is marked across volar surface. #3 handle with #15 KB.
Carpal Tunnel Release - Opencont. Operative Sequence Hemostasis: Handheld Bi-Polar Bovie
Carpal Tunnel Release - Opencont. Operative Sequence Dissection and Exposure: The incision is made across the wrist surface and base of the palm to expose the Transverse Carpal Ligament. Skin hooks, single or double toothed. Senns.
Carpal Tunnel Release - Opencont. Operative Sequence • Exploration and Isolation: • Care is taken to ID the Median Nerve so that it is not damaged during the procedure.
Carpal Tunnel Release - Opencont. Operative Sequence Surgical Repair: The Transverse Carpal Ligament is incised along its entire length with a FRESH 15 KB. Procedure can be accompanied by a Synovectomy (Surgical removal of the joint lining. Commonly performed in RA patients) Carpal Tunnel Video
Carpal Tunnel Release - Opencont. Operative Sequence Hemostasis and Irrigation: All bleeding is controlled with cautery. Use of warm Saline to irrigate.
Carpal Tunnel Release - Opencont. Operative Sequence Closure: The incision is closed in one layer. MD choice of Suture. Usually a 4-0 Nylon. A compression dressing will be applied.
Carpal Tunnel Release - Open Major Arteries: Radial and Ulnar
Carpal Tunnel Release - Open Major Veins: Ulnar veins Major Nerves: Ulnar andRadial Nerve
Carpal Tunnel Release - Endoscopic Plastic ProceduresOperative Sequence
Carpal Tunnel Release - Endoscopic Overall Purpose of Procedure: Endoscopic Carpal Tunnel release is performed to eliminate or significantly decrease the pressure on the carpal canal and the median nerve through a very small incision, utilizing a scope.
Define the procedure: With the aid of an arthroscope and arthrscopic instruments, the Transverse Carpal Ligament will be cut. Carpal Tunnel Release - Endoscopic • Carpal Tunnel Endoscopic
Craniotomy Neuro ProceduresOperative Sequence
Not to be confused • Craniotomy • Surgical opening of the skull necessary for brain surgery. The bone is replaced after surgery. • Craniectomy • Surgical opening of the skull necessary for brain surgery. The bone is not replaced after surgery.
Craniotomy Overall Purpose of Procedure: a surgical operation of the cranium resulting from removal of: Hematoma - A localized swelling filled with blood resulting from a break in a blood. Aneurysm – widening or weakening in blood vessels in the brain.
Craniotomy • Overall Purpose of Procedure cont: • Tumor removal: • There are more than 120 different types of brain tumors. • Brain tumors are often assigned different grades, ranging from a Grade I (least malignant) to Grade IV (most malignant). • It is important to note that non-malignant, or benign, brain tumors can be just as difficult to treat as malignant brain tumors.
Craniotomy • Overall Purpose of Procedure cont: • Arteriovenous malformations (AVM) - A spectrum of congenital (developmental) blood vessel malformations. An AVM occurs when brain or spinal cord arteries attach directly to veins without the blood passing through the capillary network. AVM's can cause bleeding within the nervous system (a kind of stroke), or progressive neurologic deficits, headaches or seizures.
Craniotomy • Overall Purpose of Procedure cont: • Cysts • Abscesses • Metastatic Lesions • It is very important to know the topography of the skull to help determine your approach and to help determine the amount and extent of bone removal.
Craniotomy Define the procedure: Surgery involving the removal of skull bone to gain access to the brain and the bone is put back at the end of the operation (not always).
Craniotomy Wound Classification: 1
Operative Sequence 1- Incision 2- Hemostasis 3- Dissection 4- Exposure 5- Procedure (Specimen Collection possible) 6- Hemostasis 7- Irrigation 8- Closure 9- Dressing Application
Craniotomy Instrumentation: Neuro Tray with Microsurgical Instruments. CT’s and MRI scans. Microscope and Laser if needed. Positioning: Supine with arms on arm boards. Depends on area that needs correcting. Prepping: Surgeon preference. Hibiclense or a Betadine Prep Kit. Draping: Drape according to the area of procedure. Only expose the area worked upon.
Craniotomy Begin your Operative Sequence Prior to Incision: Have Papaverine available for AVM or aneurysm case for prevention of vasospasm. Have blood product available prior to case. Incision: Must mark skin prior to incision due to the fact that landmarks will be covered when head is draped. Incise Skin and Galea (epicranial aponeurosis) with 10 KB. layer of dense fibrous tissue which covers the upper part of the cranium
Craniotomy cont. Operative Sequence Hemostasis: Handheld Bovie, Bipolar Bovie Provide Raney Clips and Raney Clip Appliers
Craniotomy cont. Operative Sequence • Dissection and Exposure: • Provide a periosteal elevator and bovie to peel scalp away from bone. • Will need to continue to coagulate galea. • Provide Fish hooks with Allis clamps and rubber bands to hold skin flap away from surgical site. • Protect skin flap with wet lap.
Craniotomy cont. Operative Sequence • Exploration and Isolation: • Place Burr holes with perforator. • Perforator will have a clutch built in so that it will retract when it meets ZERO resistance.
Craniotomy cont. Operative Sequence Surgical Repair: Bone wax will be provided to edges of cut skull bone. Provide a Dural separator. I.E. a Penfield #3 to separate the Dura from the skull. You will protect the galea with a retractor (Cushing). Pass up the Midas Rex, bone saw, to connect burr holes and TURN bone flap. (can not remove at this point)
Craniotomy cont. Operative Sequence • Surgical Repair: • You will need to provide the MD with the Penfield of choice to free bone flap completely from the dura. • BE SURE TO PROTECT THE BONE FLAP! • If you are going to replace the flap at the end of the case, you will need what you have removed. • In what situation would you not replace the bone flap? • Next we will need to prepare the bone flap for reinsertion at the end of the case. • The flap will be repositioned with surgical wire. • Pass up a drill to make holes in the bone flap for wires to pass. • Holes will be placed in flap and in surrounding bone.
Craniotomy cont. Operative Sequence • Surgical Repair: • Surgical wires can be placed the skull at this stage or at the end of case. • Provide: Gelfoam and Thrombin, Cottonoids, Raytex’s, etc to be sure all bleeding is under control. • Hand sterile blue towels to MD to cover wires if placed prior to rest of case. • We now prepare to open the Dura. • To open the Dura, we will pass up the Dural Hook to lift it up and away from the cortex. • Hand 15 Kb to MD to nick the Dura. • Hand small scissors of choice to MD to continue opening the Dura.
Craniotomy cont. Operative Sequence • Surgical Repair: • MD may need bipolar forceps or hemoclips to maintain hemostasis. • MD will need to retract the Dura. Have fish hooks ready. • Provide damp sponge or damp cottonoid patty to keep Dura moist at all times. • Continue procedure based on pathology. • If presented with an aneurysm: • Have mico-suction available to clear clot away. • Pass up self retaining retractor of choice if needed (Greenburg). • The brain's lobes are gently retracted until the location of the aneurysm is reached, using a surgical microscope and microsurgical instruments.
Craniotomy cont. Operative Sequence • Surgical Repair: • Aneurysm:The paper-thin aneurysm is carefully freed from the scar tissue surrounding it, and its junction with the brain's blood vessels is identified. One of various kinds of clips is placed across the base of the aneurysm and is adjusted until its position is accurate. This allows the aneurysm to collapse, but spares the essential blood vessels around it. • At times the aneurysm will rupture again while surgery is taking place. The surgeon then carefully tries to control the hemorrhage while continuing the delicate clipping procedure.
Craniotomy cont. Operative Sequence • Surgical Repair: • Tumor Removal: • Once the Dura is exposed, an ultrasound probe is used to confirm the location and depth of the underlying tumor and help the surgeon plan his approach. • The tumor is carefully dissected from normal brain tissue with microsurgical instrumentation. • For an intracranial tumor, a small incision is made through the surface of the brain and into brain tissue until the tumor is reached. Ultrasound frequently is used to monitor the tumor's removal.
Craniotomy cont. Operative Sequence • Surgical Repair: • Tumor Removal cont: • instrumentation may be used by the neurosurgeon to visualize, cut into, and remove the tumor, include a surgical microscope or special magnification glasses, a surgical laser that vaporizes the tumor and an ultrasonic tissue aspirator that breaks apart and suctions up the abnormal tissue. • At this time the biopsy is sent to the laboratory for analysis. • Unlike elsewhere in the body, where some extra tissue around a tumor may be surgically removed "just to be sure," only tissue that can clearly be identified as abnormal may be removed from the brain-and even then only if its removal is possible without devastating consequences.
Craniotomy cont. Operative Sequence Hemostasis and Irrigation: All bleeding is controlled with cautery. Use of warm Saline to irrigate. Provide chemical hemostatic of choice. I.E. Surgicel.
Craniotomy cont. Operative Sequence Closure: Close Dura with suture on a small, cutting needle. After the dura has been stitched closed, the piece of bone is replaced and sutured/wired into place. An ICP (intracranial pressure) monitoring device may then be implanted. Closure of muscle and galea layer with suture of choice. Skin staples or suture for scalp. If a drain is required, provide Nylon or Prolene drain stitch.
Craniotomy cont. Operative Sequence • ICP monitoring : • Intracranial pressure monitoring is a device, placed inside the head, which senses the pressure inside the brain cavity and sends its measurements to a recording device. • The intraventricular catheter is thought to be the most accurate method.
Craniotomy cont. Operative Sequence • ICP monitoring : • To insert an intraventricular catheter, a burr hole is drilled through the skull and the catheter is inserted through the brain matter into the lateral ventricle, which normally contains liquid that protects the brain and spinal cord (cerebrospinal fluid). Not only can the intracranial pressure (ICP) be monitored, but it can be lowered by draining cerebral spinal fluid (CSF) out through the catheter.
Craniotomy cont. Operative Sequence • ICP monitoring : • This catheter may be difficult to place with increased intracranial pressure, since the ventricles change shape under increased pressure and are often quite small because the brain expands around them from injury and swelling. • Normally, the ICP ranges from 1 to 15 mm Hg.
Craniotomy cont. Operative Sequence • ICP monitoring : • Raised intracranial pressure means that both nervous system (neural) and blood vessel (vascular) tissues are being compressed. If left untreated, it can result in permanent neurologic damage. In some cases, it can be fatal.
Lumbar Discectomy • Video
Lumbar discectomy is a surgical procedure to remove part of a problem disc in the low back. The discs are the pads that separate the vertebrae. This procedure is commonly used when a herniated, or ruptured, disc in the low back is putting pressure on a nerve root.