Download
1 / 62
780 likes | 1.2k Views
Antiphospholipid Syndrome. Prof. Dr. Suchitra N. Pandit MD, DNBE, DFP, FRCOG, FICOG, B.Pharm Consultant Obstetrician & Gynaecologist Kokilaben Dhirubhai Hospital, Mumbai ,India Clinical secretary –MOGS, Vice President - FOGSI (2008-09)

E N D
Prof. Dr. Suchitra N. Pandit MD, DNBE, DFP, FRCOG, FICOG, B.Pharm Consultant Obstetrician & Gynaecologist Kokilaben Dhirubhai Hospital, Mumbai ,India Clinical secretary –MOGS, Vice President - FOGSI (2008-09) Chairperson -Young Talent promotion committee FOGSI (2003-07)
Antiphospholipid ( APLA ) syndrome • Antiphospholipid syndrome (Hughes syndrome) is a disorder of immune system ,characterised by excessive clotting of blood ,thrombocytopenia & /or adverse pregnancy outcomes • Body recognizes negatively charged phospholipids on cell membrane as foreign & produces antibodies against them leading to an acquired autoimmune thrombophilia • Patients have laboratory evidence for antibodies ( IgG, IgM or IgA ) against phospholipids or phospholipid-binding protein cofactors in their blood
How many types of APLA syndromes are there • A.) One • B.) two • C.) Three • D.) Four
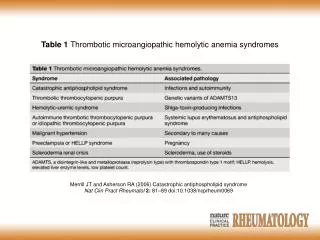
Antiphospholipid antibody syndrome (APLA) • Primary antiphospholipid syndrome (PAPS) - when APS occurs in the absence of any other related disease (LA, ACL antibodies in patient’s serum). • Secondary antiphospholipid syndrome - when APS coexists with other diseases such as SLE I • In catastrophic APLA (rare ), APS leads to rapid organ failure due to generalised thrombosis & a high risk of death • Other rare antibodies to phosphotidyl ethanolamine & phosphotidylserine are also associated with it
Thrombophilic defects either acquired or inherited
Thrombophilia - tendency to thrombosis Lupus anticoagulant antibodies Acquired APLA Anticardiolipin antibodies • Myeloprolipherative diseases • Malignancy • Paroxysmal nocturnal Haemoglobinuria • Nephrotic syndrome
Inherited • Hyperhomocysteinemia (C677T) mutation • Factor V Leiden mutation (A506G) mutation • Mutation in prothrombin ( G 20210 A) • Prothrombin II (PTII) mutation • Protein S deficiency • Protein C deficiency
All these conditions should be investigated for APLA except : A.) Early onset severe preeclampsia B.) Arterial or venous thrombosis C.) Unexplained fetal growth restriction D.) Gestational Diabetes
Primary antiphospholipid antibody syndrome Presentation may be totally asymptomatic or in a classical manner : Various clinical presentations : • Recurrent pregnancy loss • Unexplained second or third trimester loss • Early onset severe preeclampsia • Arterial or venous thrombosis • Unexplained fetal growth restriction • Prolonged coagulation studies • Autoimmune diseases • Cardiac valvular diseases • Neurological disorders • Thrombocytopenia
Diagnosis of APLA Challenging !!! • Due to fluctuating titers of the antibodies, • Lack of agreement between laboratories concerning standardization of the assays • Debates among researchers & clinicians concerning which antibodies to measure.
Which is not an APLA antibody ? A.) Anti Ro B.) Lupus Anticoagulant (LAC) C.) Anticardiolipin Antibodies (ACL) D.) Anti insulin antibodies
Which are the Antibodies • Lupus Anticoagulant (LAC) • Anticardiolipin Antibodies (ACL) • Anti Beta 2 glycoprotein antibodies • Other antibodies
Lupus anticoagulant ( LAC) • LAC is characterized by a prolonged partial thromboplastin time & paradoxically the so-called ‘anticoagulant’ is a powerful thrombotic agent in vivo • Higher thrombotic potential than ACL when present alone • LAC interferes with platelet function, causing aggregation & thrombosis & also interferes with endothelial function, causing procoagulant activation & thrombosis • Prevalence of LAC in low risk population is < 1% Bad obstetric history - 9.1% Early pre eclampsia - 16%, Abruption - 33% Systemic lupus erythematosus - 34%
Patient typically has a prolonged APTT that does not correct in 80:20 mixture with normal human plasma • Prolonged Dilute Russel viper venom time (DRVVT), Kaolin clotting test (KCT),(TDT/DTT) or prothombin time • Due to heterogeneous nature of LA ,minimum of 2 tests required, 6 weeks apart & should be positive each time showing persistent positivity to confirm diagnosis of APLA Caution : patients with transient positive tests (due to infection etc) can be diagnosed as positive.
Lupus anticoagulant (LAC) Prolongation of which of these tests is most sensitive for LAC ? A.) Activated partial thromboplastin B.) Dilute Russel Viper venom C.) Kaolin clotting time D.) Partial Thrombin time
Anticardiolipin Antibodies • Were thought to react against cardiolipin but it is now thought to interact with B2GP1 • 85% of APS pts have both LA & aCL • These can be detected using an (ELISA) • Screens for the presence of β2 glycoprotein 1 dependent anticardiolipin antibodies (ACA) • A low platelet count & positivity for antibodies against β2-glycoprotein 1 or phosphatidylserine may also be observed in a positive diagnosis
Anti Beta 2 GP1 • Discovered after LA & ACL • Found without other two in 11% of APS pts & commonly with others. • Binds to B2GP1 disrupting f(x) • B2GP1 has anticoagulant activity through the inhibition of the conversion of prothrombin-thrombin, regulation of protein S, & /or activation of platelets.
Sapporo criteria International Consensus Conference held in Sapporo (’98) Clinical criteria of ( APAS ) Thrombosis, one or more confirmed episodes of venous, arterial, or small vessels disease ‘ Coexisting inherited or acquired thrombotic risk factors are not reasons for excluding patients from a diagnosis of APS trials.’
Sapporo Criteria (updated) Pregnancy criteria : • One or more unexplained fetal deaths > 10 wks of pregnancy • One or more preeclampsia / eclampsia or placental insufficiencies occurring before 34 weeks . • Three or more unexplained consecutive spontaneous abortions < 10 weeks Laboratory criteria • LAC defined by a functional, clot-based assay (ISTH guidelines) • ACL (IgG or IgM) antibody • Anti-b2 glycoprotein I ,IgG or IgM antibody Miyakis, et al., J. Thromb. Haemost.,2006; 4: 295-306.
The International Consensus Statement Definite CAPS diagnosis requires: • Vascular thrombosis in three or more organs or tissues & development of manifestations simultaneously or in < a week & small vessel thrombosis in at least one organ or tissue • Lab. confirmation of presence of aPL • Some serological tests for syphilis may be positive in aPL- positive patients if it is positive) although more specific tests for syphilis that use recombinant antigens are negative • Transient elevations common. Elevations common in autoimmune disease & infections ex. HIV, Hep C, syphilis
Interference with a.)Soluble coagulation factors Protein C/S pathway inhibition; fibrinolysis inhibition b.) Coagulation cells: Induction of a pro-adhesive, pro-inflammatory & pro-coagulant endothelial phenotype ;induction of a procoagulant phenotype in monocytes Interference with : a.) Trophoblast cells: Reduction of proliferation & differentiation; Gonadotrophin secretion impairment Principal pathogenic mechanisms mediated by APL
Pregnancy losses classified as : • Occult (preclinical or chemical) pregnancy loss prior to missed menses. (40% of implantation embryos) • Early pregnancy loss before 12 wk. (13%) • Late pregnancy loss after 12 wk. (1%)
Causes of pregnancy loss Chromosomal 55%of occult & early losses 5% of recurrent losses. Environmental hormonal anatomical Immunological 45% of early losses 95% of late losses
Aneuploidy Aneuploid fetus risk in women > 35yr. age Standard of care is to offer genetic amniocentesis for all pregnant women older than 35 years 1/80 Inherent risk of fetal loss after amniocentesis 1/200
What is Recurrent pregnancy loss ? What actually causes it ?
Definition A recurrent pregnancy loss (RPL) is 3 or more consecutive, spontaneous pregnancy losses, under 20 week gestation from the last menstrual period by the same partner. • Primary recurrent pregnancy loss" refers to couples that have never had a live birth • “Secondary RPL" refers to those who have had repetitive losses following a successful pregnancy
Pregnancy loss in the APLA syndrome - A possible thrombogenic mechanism • Levels of annexin V, a phospholipid-binding protein with potent anticoagulant activity, are markedly reduced on placental villi from women with APLA • APL antibodies reduce the levels of annexin V & accelerate the coagulation of plasma on cultured trophoblasts & endothelial cells. • Reduced annexin V levels on vascular cells may be an important mechanism of thrombosis & pregnancy loss in APLA syndrome. Jacob Rand, Xiao-Xuan Wu, H. Andree, CJ. Lockwood, Seth Guller, J Scher, Peter Harpel, -N Engl J Med ; 337:1630-1631, 1997
Pregnancy loss in autoimmune connective tissue disorders (CTDs) • Adverse outcomes like IUGR, prematurity, recurrent pregnancy loss & stillbirth are common • Systemic lupus erythematosus (SLE) is prototype , others are rheumatoid arthritis, scleroderma, Behcet’s disease & Sjogren’s syndrome • Recent studies show anti-Ro/SSA antibody as a possible factor for unexplained pregnancy loss in SLE. • Antibody is directed against cellular ribonucleoprotein complexes which is present in serum of > 10% pts of CTDs. • It is associated with neonatal lupus & congenital heart block showing passively acquired autoimmunity
How do you proceed ? • Interview the couple together • History of the case is very important • Clinical examination • Investigations as per the history • Reassurance & counselling • Treatment plan : Drugs, maternal & fetal surveillance , dealing with complications • Timely referral to a tertiary centre
Special Investigations • LAC tested by prolonged coagulation time (inhibition of phospholipids) • APTT , KCT , TTIT • Most accurate - Dilute russel viper venom test (DRVVT) • ACL - ELISA - IgG (GPL) IgM (MPL) • IgG/ IgM isotypes of anticardiolipin & antiphosphotidyl serine antibodies • In c/o low titres-repeat after 6-8wks (can revert to normal) • Transient low titres can be found in viral fever • If autoimmune disorders are suspected ANA, anti –nDNA, antiSm, anti-Ro/SSA antibody, anti La (SSP)
General guidelines for anticoagulation in Pregnancy with APS leading to recurrent pregnancy loss So how does one manage the drug treatment in pregnancy ? Very controversial issue !
Commonly used Drugs • Steroids : Reduces ACA, normalises prolongation of invitro coagulation • Complications : ? perinatal outcome preterm labour, preeclampsia • Low dose Aspirin (LDA) : Selective inhibition of Thromboxane A2 No effect on PGI2 • Azathioprine • Warfarin
Which is the commonly used drug for APLA ? A.) Progesterone B.) Folic acid C.) Low dose Aspirin D.) RU- 486
Unfractionated Heparin (UFH) • Potentiates complex formation with AT III + factor VII A XII A & thrombin • Complications : Reduces platelet bleeding & B.M.D. Low molecular weight Heparin (LMWH) • Once daily dose, less monitoring • Lesser osteopenia, does not cross placenta • Cost factor !!
Trials • Heparin vs Aspirin + prednisolone Live birth 75% Pre-eclampsia, preterm delivery more in latter group • L.S. + LDA Vs Heparin + LDA (n=20) • No placebo • Large multicentric trials needed Cowchock et al .1994
Randomised controlled trial of LDA versus LDA plus heparin in pregnant women with APS • 90 women with APS were randomized into two groups with 1st group receiving 75mg of LDA & 2nd group LDA & Heparin 5000u subcut, every 12 hourly • Outcomes measured were number of live births & miscarriages • LDA group had 19 live births & 26 miscarriages • LDA + heparin group had 32 live births & 13 miscarriages • Significant (p=0.01) improvement in outcomes with heparin R. Rai, H.Cohen et al..,BMJ. (1997 )
Antiphospolipid antibodies Presence of Antiphosholipid antibodies may cause recurrent pregnancy loss • Are antibodies directly responsible ? • Should all women with APA be treated ? • How do you treat a women with positive APLA ?
Controversies surrounding treatment for pregnancy loss • Evidence-based medicine (EBM) has not succeeded in giving patients & physicians the data they need to choose (or not choose) a therapy in the field of pregnancy loss
Women with APLA are advised to take LDA & to start LMWH Rx after pregnancy is diagnosed (80% success) • In case of H/o thrombotic symptoms, Warfarin is used as anticoagulant .Maintain INR between 3.0 - 4.0. • Patients with APLA have minor elevations of PT & are difficult to manage with warfarin. • During pregnancy, LMWH & LDA are preferred to Warfarin (teratogenic effects ) • If previous H/o thrombosis use LMWH in therapeutic doses throughout pregnancy :dose 1mg/kg subcut. • If UFH is used dose is 10,000 u 12 hourly
Since APLA reacts with phospholipids both aPTT & PT can be affected. If UFH used to anticoagulate patients with APLA monitor heparin levels ( 0.35 - 0.70 anti-Xa units 6 hours post injectiont ). • With LMWH , monitoring is easier : predictable dosing & anticoagulant effect . Measure LMW heparin levels in these patients for long term Rx (0.7 - 1.0 anti-Xa units) • Perform prothrombin & proconvertin times ("P&P") to follow anticoagulation. Being less dependent on phospholipids & one can monitor therapy. • If miscarriage occurs with heparin & aspirin & there is a pregnancy again IVIG can be tried (RCT did not show benefit) • In refractory cases plasmapheresis may be used
ACCP Guidelines : Pregnancy & APL - Bates, et al., Chest, 2004; 126: 627S - 644S
Management of pregnant women • Surveillance depends on past obstetric history • LDA preconception & LDA + LMWH has 80% success rate for treatment of APLA ( Feinberg et al,’ 97 ). • Refer preferably to a tertiary centre with a neonatal backup • Team effort including an obstetrician , hematologist, physician, & neonatologist • Vigilant monitoring • B.P, platelets, complement levels , renal function test (to asses target organ damage )
Care of the fetus • Surveillance depends on past obstetric history • 1st trim U.S.G : viability & dating , nuchal & nasal bone • U.S.G at 19 weeks & serial scans with doppler for early diagnosis of IUGR & waveform abnormalites • Inj Betamethasone 2 doses for enhancing lung maturity • Timely delivery in a centre with a good neonatal backup
Future Possibilities • PAPRE warfarin intensity • PRECLUDE primary prevention • More frequent use of LMWH, IVIG
What to do with the patient with APLA but no thrombotic manifestations ? • Although some of these patients are at risk, especially those with SLE, many will never develop thrombosis • The current recommendation would be to do very careful search for thrombosis. Brain MRI in patients with SLE & in patients with any neurological symptom • If this work-up is negative follow the patient very closely Does immunosuppression work ? APLA seems like an autoimmune disease, but immunosuppression does not prevent recurrent thrombosis, fetal loss, or neurological syndromes & so no role in the Rx of thrombotic APLA
In"catastrophic APLA" plasmapheresis may play a crucial role. • Low intensity anticoagulation with warfarin appears to be mostly effective in APLA (except patients with venous thrombosis) • Many patients will fail low intensity warfarin & need more aggressive anticoagulation. • Heparin anticoagulation appears more effective.Arterial Thrombosis: Warfarin to an INR of 2.0 - 3.0 Venous Thrombosis: Warfarin to an INR of 3.0 - 3.5. Patients who "break through" warfarin should receive heparin.