Download
1 / 33
330 likes | 341 Views
Lyme notifications – USA. 6 th most common notifiable disease in 2011. http://www.cdc.gov/lyme/stats/chartstables/reportedcases_statelocality.html http://www.cdc.gov/lyme/stats/chartstables/incidencebystate.html. Reservoir competence High –White footed mouse Low – Deer Mouse

E N D
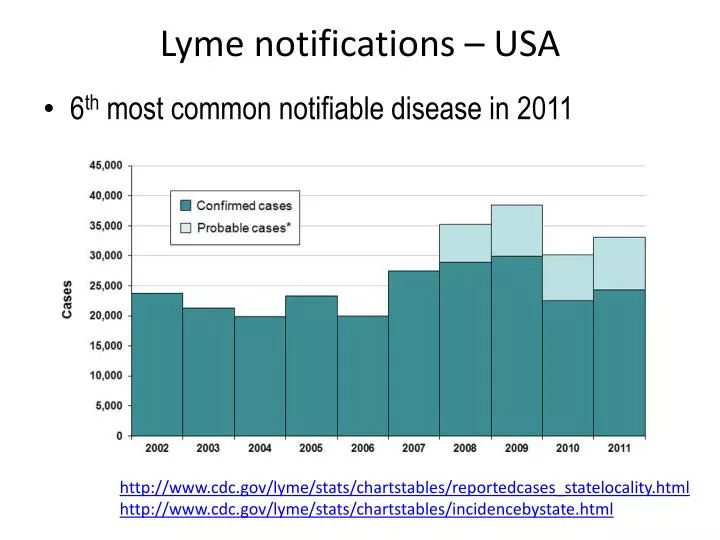
Lyme notifications – USA • 6th most common notifiable disease in 2011 http://www.cdc.gov/lyme/stats/chartstables/reportedcases_statelocality.html http://www.cdc.gov/lyme/stats/chartstables/incidencebystate.html
Reservoir competence High –White footed mouse Low – Deer Mouse Refractory – Deer; Lizard Preferred Hosts North – White footed mouse South – Lizard West – Lizard
Lyme Disease Europe • Annual cases - 65,500 • <1 / 100,000 population - 350 / 100,000 population • Highest in residents of northern & central countries • Focal pattern of distribution related to suitable tick habitat • hotspots where more than 100 / 100,000 population per year • Parts of Slovenia, Germany, Austria, Baltic coastline of southern Sweden, and some Estonian & Finnish islands Euro Surveill. 2011;16(27):pii=19906. Available online: http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=19906
Lyme Disease Australia • Handful of Lyme like cases Hunter, Central NSW Coast, NSW south coast 1-3 • Culture positive case B.burgdorferi & B.garinii however as well being bitten by a tick had travelled to USA & central Europe4-5 • Seroprevalence in blood bank population and non endemic regions – 2-4% • 2011 NSW – expert panel review of suspected caes 1. MJA 1982;1:139, 2. MJA 1986;145:364; 3. MJA 1986;144;724 4. CDI 16/24;516; 5. MJA 1998;168:500
Human Infection • Early localised (Stage I) - (requires > 24 hours attachment) • Dermal infection - erythemamigrans (80% of patients) • ± Constitutional signs • Early disseminated (Stage II) - hematogenous +/-lymphatic dissemination (weeks to months) • 2°EM lesions (multiple) • Neurological (15%) – lymphocytic meningitis; VII N palsy, painful meningoradiculitis (Bannwarths syndrome) • Cardiac (5%)- high grade AV conduction defects, myopericarditis • Joints – recurrent brief attacks in 1-3 joints • Late infection (Stage III) - months to several years • 60% rheumatological involvement • 5% chronic neuroborreliosis - PN, encephalopathy • Rarely acrodermatitischronicaatrophicans in US
Clinical Manifestations of Confirmed Lyme Disease Cases US 2001-2010
Laboratory Diagnosis • Low numbers of Lyme spirochaetes in any clinical sample necessitates amplification for detection • Culture • PCR • Serology
Borrelia Culture • Media: Barbour Stoenner-Kelly (BSK) with rabbit serum & albumin • Incubate 30°C microaerophilically • Slow growth – days to weeks • Cultivable samples: • ticks • infected reservoirs • human (EM skin biopsy, blood, synovial tissue, CSF) • Cultures positive mainly from early LD (EM & neuroborreliosis) • Limited clinical utility
Molecular Detection • No. of spirochaetes is low in clinical specimens • Sample types – skin, blood, CSF, synovial fluid • Targets include – flaB, 16SrRNA, recA, p66,ospA, 5SrRNA-23SrRNA gene spacer region • Australia PCR - PaLMs: B Hudson – nested PCR targeting flagellin gene • Only accepts skin/CSF – need to contact lab
Approximate Yields Culture v PCR* Aguero-Rosenfeld et al Clin Micro Rev 2006:18;484 * Over 30 studies reviewed; positive correlation with multiple EM and other evidence of dissemination… ………. < 1 spirochaete/ml whole blood in over 70% of patients
Differential Expression of Borrelial Genes • Complex antigenic composition • Differential expression of many genes between tick and mammal environment • Antigenic differences among the different species of B.burgdorferisensulato
Important antigens • Flagellar protein Flagellin (41kD) - FlaB • Immunodominant • Early IgG / IgM response • BUT – cross reactive • with other bacteria especially when denatured for immunoblots • mammalian tissue –synovium, neural & cardiac tissue • Flagellar outer sheath protein (37 kD) - FlaA • Also immunodominant especially in early disease
Serology contd Outer surface proteins - Osp A-F • OspC (21–25kD) • Immunodominant • Expressed with tick feeding • Highly passaged organisms do not express OspC • Heterogeneous amongst and within genospecies • Virulence factor – infectivity and invasiveness • Antibodies bactericidal • pepC10 = synthetic peptide = Conserved C terminal region • OspA (31kD) • 25°C unfed tick mid gut • Not expressed early • Detected during late infection • Antibodies bactericidal
Lyme Vaccine • Recombinant OspA (LYMErix; GlaxoSmithKline, NY) 1998 • anti-Borrelia antibodies - taken into the tick’s gut during feeding • These abs attack the spirochete, thereby ending the cycle of infection • Effectiveness rivalled that of simple environmental precautions • Withdrawn 2002 - economic reasons; long-term efficacy doubts, no recommendations for children or arthritis
Serology contd • Early human infection • FlaB (41 kDa) • Osp C (23 kDa) • VlsE = Vmp-like sequence expressed lipoprotein (34kD) • Surface exposed lipoprotein from a linear plasmid • Variable and invariable domains • C6 = invariable of VlsE is highly immunogenic • BmpA - Borrelia Membrane Protein (39kD) • Late: marked adaptive immune response with an expanding antibody profile
Serological Assays • At least 80 different commercial assays – FDA approved • Most use B31 type strain as a source of antigen • Whole cell sonicates- IgG, IgM, IgG/IgM • Low passage isolates • Sensitivity if < 1 week = < 50% • Sensitivity increases with time • Invariably positive with late disease (arthritis) • Lack specificity – cross reactions with heat shock proteins, flagellar antigens • Recombinant antigens: e.g Bmp A (39 kDa) • Purified antigens– flagellar components • Single synthetic peptide derived from VlsE (C6 peptide) • Vmp-like sequence expressed protein (34kD)
Limitations • Lack of standardisation • Variation in antigen used in EIA • Immunoglobulin class • FDA approved kits - not standardised against a panel of well characterised sera • Duration of infection • Disease manifestation (disseminated v localised) • Properties of B.burgdorferi strain
False Positives • Tick-borne relapsing fever • Syphilis • Anaplasmosis: granulocytic ehrlichiosis • Leptospirosis • Some autoimmune disorders (e.g., lupus) • Bacterial endocarditis • Infection with Helicobacter pylori, Epstein Barr virus, or Treponemadenticola(bacteria found in the mouth that can cause gum disease and/or infection after dental procedures)
Incidence/Pretest Likelihood Predictive Value • Incidence 1% • Assume Sens 98% Spec 98% • NPV = 970/970 =100% • PPV = 10/30 =33% • (67% false positives ) • Incidence 40% • Assume Sens 98% Spec 98% • NPV = 588/596 =99% • PPV = 392/404 =97% Even with a good test, false positives occur when pretest likelihood is low
CDC Criteria for WB interpretation • IgM WB • Engstromet al - strain 297 • 2 of 3 immunoreactive bands • FlaB (41 kDa), BmpA (39 kDa ), and OspC (23/4 kDa ) • Can only be used in the first 4 weeks of illness • IgG WB • Dressler et al – strain G39/40 • 5 of 10 bands • OspC (21kD), FlaB (41kD), 93 (P83/100), 66kD, 58kD, 45kD, BmpA (39kD), 30kD, 28kD, 18kD • Band number increases with neuroborreliosis or late LB • Can be used early or late in illness • Allows detailed examination of the immune response over time MMWR 1995;44:590-591
IgM WB 1. 41-kDa, 39-kDa protein, OspC 2. early LB with EM 3. early disseminated LB with multiple EM lesions IgG WB 1. significant antigens 2. early disseminated LB with neurological involvement 3. Lyme arthritis 4. 3 doses OspA vaccine (31kD)
IgG WB ICPMR • Whole cell organism electrophoresed and transferred to nitrocellulose • B.burgdorferi and B.afzelii • IgM WB not offered; EIA pos samples only tested • Most common bands - 41kDa (flagellin) and 58kDa • Nearly 42% have no bands • 54% 1-4 bands • 4% (71) have ≥ 5 bands (average from 1994 – 2011).
Unorthodox assays • CD57 is on NK cells • Lyme urine antigen tests (LUAT) • Immunofluorescent staining for cell wall--deficient forms of Borreliaburgdorferi(QRIBb) • Lymphocyte transformation tests (LTT) • PCR on inappropriate specimens such as blood and urine or • Interpret Western blots using criteria that have not been validated and published in peer-reviewed scientific literature. MMWR February 11, 2005 / 54(05);125 CVI 2009, 16:1249–1250 Marques A, et al
Challenge: increase sensitivity, maintain specificity, simplify complexity • EIA - C6 (VlsE) 1 • Results similar to 2 tier testing • More sensitive marker of early disease (I and II) • Less sensitive in chronic disease (III) – a few patients lacked reactivity with C6 peptide • Less specific than 2 tier testing • 2- tier approaches increase specificity • IgM WB • Sensitive in early disease • Subjective and suffers false positives • CDC – illness <1 month (reduces sensitivity in stage 2 acute neuroborreliosis CID 2008 ;47:188 Steere et al CID 2010;50:20 Branda et al CID 2011;153:541 Branda et al
Alternative 2 –tier strategies • Standard 2 tier: WC EIA followed by IgM / G WB • 2-EIA: WC EIA followed by C6 EIA • C6 alone 2-EIA strategy realises sensitivity benefits of C6 in stages I and II minimizes complexity/subjectivity and maintains specificity of standardised 2 –tier Branda JA et al CID 2011;53:541-547
Options: • 2 step EIAs – WC EIA followed by C6 EIA • C6 assays could replace 2 step testing altogether because of increased sensitivity • Add recombinant antigens & peptides to immunoblots • Need further evaluations using well characterised LB sera at different stages of illness • Need to ensure state of art testing algorithms • Develop an Australian Laboratory Case Definition • No Australian QAP programme CID 2008:47 :196
Independent Appraisal and Review of ILADS2004 ‘Evidence-based guidelines for the management of Lyme disease’8 December 2010 The ILADS guidelines are poorly constructed and do not provide a scientifically sound evidence-based approach to the diagnosis and care of patients with Lyme borreliosis. The ILADS working group does not provide evidence that it used a Cochrane based or similar approach in developing the guidelines. Some references do not provide evidence to support statements for which they were cited in the guidelines. Some good-quality peer-reviewed articles are selectively quoted, using sub-group analyses without regard for the broader findings of the full studies. Some references were published in a n advocacy group-sponsored journal that was not Medline -listed, others are available only as conference / symposium abstracts or are unpublished. Some reference citations are inaccurate, demonstrating poor attention to detail “Evidence-based guidelines for the management of Lyme disease” (Cameron et al. Exp Rev Anti-infect Ther 2004;2:S1-13).