Download
1 / 15
170 likes | 301 Views
The Physiology of the Proximal Tubule. Structure of the Proximal Tubule. The proximal tubule receives the ultrafiltrate from the glomerulus.

E N D
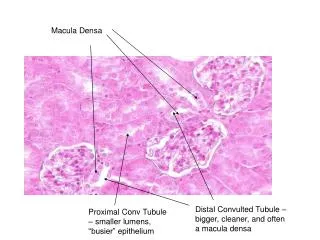
Structure of the Proximal Tubule • The proximal tubule receives the ultrafiltrate from the glomerulus. • The proximal tubule is an epithelium consisting of a single layer of cells that are oriented so that they separate the luminal fluid that eventually becomes urine and the interstitial fluid. • The membrane surface in contact with the luminal compartment (apical membrane) has microvilli (brush border), and the surface in contact with the interstitium (basolateral membrane) has multiple infoldings to maximize the total surface area available for transport.
Transport can be divided into active (transcellular) and passive (paracellular) transport. • The early part of the proximal tubule (proximal convoluted tubule) is located in the cortex of the kidney. • The proximal convoluted tubule has a higher transport rate than the proximal straight tubule and has a higher energy demand. • The cortex of the kidney receives the bulk of the renal blood flow and so can provide more energy to sustain the metabolic demand of the proximal convoluted tubule cells as well as carry the reabsorbed fluid and solutes into the bloodstream. • The proximal straight tubule is located in the outer medulla and is more susceptible to ischemic damage, resulting in acute tubular necrosis.
Transport in the Proximal Tubule • Transport in the proximal tubule is driven primarily by Na/K/ATPase, which is located in the basolateral membrane of the cell. • This enzyme maintains a low intracellular sodium concentration, which can then be used by transporters located in the apical membrane for secondary active transport
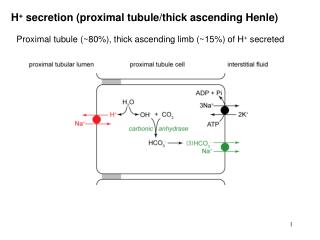
Bicarbonate Transport • Sodium-hydrogen exchanger (NHE3) exchanges one hydrogen ion for each sodium ion that enters the cell and is the first step in the reabsorption of bicarbonate. • Once the hydrogen ion enters the lumen of the tubule, it combines with a bicarbonate ion to form carbonic acid, • In the presence of carbonic anhydrase, the carbonic acid is converted to carbon dioxide (CO2) and water, which then enter the cell. • Intracellular carbonic anhydrase then catalyzes the recombining of the CO2 and water into carbonic acid. • The bicarbonate then exits the cell via the basolaterally located sodium-bicarbonate cotransporter (NBC1). • The proton can then be transported again through the apical membrane. • In addition to the sodium-hydrogen exchanger, there is a proton pump (H+-ATPase) located in the apical membrane that also secretes hydrogen ions through direct hydrolysis of ATP.
Sodium Chloride Transport • The sodium-hydrogen exchanger is used to transport sodium chloride actively through the tubule cell. • This occurs because the intracellular pH rises after the hydrogen ion is transported into the lumen, providing a pH gradient for the chloride-base exchanger to allow the entry of a chloride ion into the cell through the apical membrane. • Because there is more bicarbonate than chloride reabsorbed, there is a favorable gradient for the reabsorption of chloride through passive, paracellular junctions.
Glucose Transport • Early in the proximal tubule, there is a sodium-glucose cotransporter (SGLT2) that transports one sodium ion and one glucose molecule. • As the proximal tubule intracellular glucose concentration rises, glucose diffuses out through the basolateral membrane by means of a facilitative transporter (GLUT2). • This process is saturable. • If the tubule is presented with more solute than it is capable of transporting, reabsorption is incomplete. • This is the basis for the osmotic diuresis found in the diabetic patient when the serum glucose concentration is elevated and exceeds the transport maximum for glucose.
Phosphate Transport • Phosphate homeostasis in the body is regulated primarily by alterations in proximal tubule transport of phosphate. • Under normal conditions, about 85% of the filtered phosphate is reabsorbed by the proximal tubule by means of the sodium-phosphate cotransporter (NaPi2) • Parathyroid hormone (PTH) promotes renal excretion of phosphate. • It stimulates endocytosis of the NaPi2 cotransporters from the apical membrane of the proximal tubule cells.
Secretion in the Proximal Tubules • A number of organic molecules are actively secreted in the proximal tubule. • The mechanism of secretion is similar to that of reabsorption, except that the transporters for uptake are located in the basolateral membrane. • The principal molecules that are secreted include creatinine and many drugs (e.g., penicillins).
Transport of Water • Active transport of solutes in the proximal tubule leads to an intraluminal fluid that is hypo-osmotic compared with the blood. • The proximal tubule has a very high osmotic water permeability due to the presence of aquaporin in its apical and basolateral membranes. • The high permeability allows for the rapid movement of water and the nearly iso-osmotic reabsorption of the glomerular filtrate.
Metabolic Functions • Ammoniagenesis • The proximal tubule can reabsorb the bulk of the filtered load of bicarbonate but can not excrete acid. • Can only conserve the bicarbonate that is already in the body. • Ifthe body has accumulated acid (or has lost base equivalents in diarrhea), it must generate new bicarbonate.
It does so by generating ammonia, which is then secreted into the lumen of the tubule for eventual excretion in the form of ammonium chloride. • The enzymes for ammoniagenesis are located in the proximal tubule and are under the control of the acid-base balance. • Under conditions of acidosis, the kidney can more than double its production of ammonia so that the body can repair the base deficit that has accumulated.
Gluconeogenesis • The proximal tubule has all the enzymes for gluconeogenesis. • The rate of glucose production by the kidney is second only to that by the liver. • Vitamin D Synthesis • The proximal tubule is the site in the kidney for the 1α-hydroxylase enzyme in the synthetic pathway for vitamin D activation. • This enzyme is primarily under the control of PTH.
Regulation of Proximal Tubule Transport • When the body becomes volume depleted, a number of events occur that prevent the ongoing loss of fluid through the kidney. • First, the kidney secretes renin, leading to the production of angiotensin II. • This causes vasoconstriction of the efferent arteriole and increasing the filtration fraction. • As a result, the blood in the efferent arteriole has a higher than normal protein concentration. • Thus, the peritubular capillaries have a higher oncotic pressure, which enhances the movement of fluid from the interstitium to the circulation, improving reabsorption of the glomerular filtrate by the proximal tubule. • The renal nerves are activated during volume depletion, and the norepinephrine causes the tubule to increase its transport rate.