Download
1 / 1
10 likes | 100 Views
Intermittent Ischemia due to an Unlikely Toxin. Beth Kushner D.O PGY 1 & Nilesh Patel D.O. Chief Complaint: My stomach is going to explode.

E N D
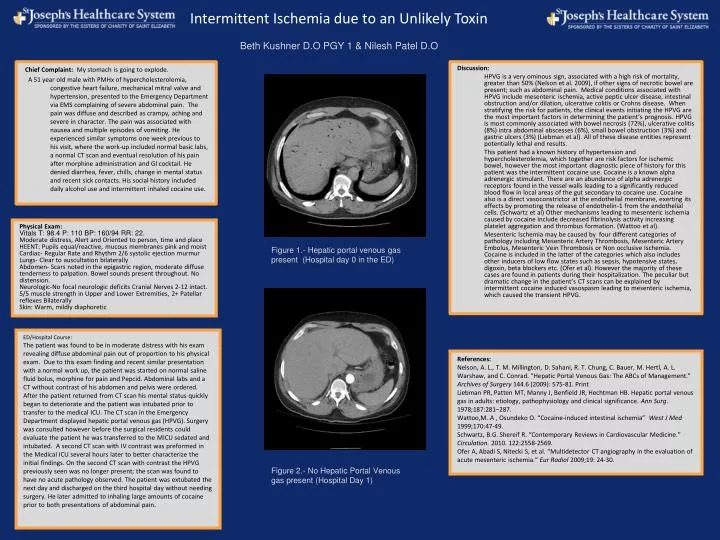
Intermittent Ischemia due to an Unlikely Toxin Beth Kushner D.O PGY 1 & Nilesh Patel D.O Chief Complaint: My stomach is going to explode. A 51 year old male with PMHx of hypercholesterolemia, congestive heart failure, mechanical mitral valve and hypertension, presented to the Emergency Department via EMS complaining of severe abdominal pain. The pain was diffuse and described as crampy, aching and severe in character. The pain was associated with nausea and multiple episodes of vomiting. He experienced similar symptoms one week previous to his visit, where the work-up included normal basic labs, a normal CT scan and eventual resolution of his pain after morphine administration and GI cocktail. He denied diarrhea, fever, chills, change in mental status and recent sick contacts. His social history included daily alcohol use and intermittent inhaled cocaine use. Discussion: HPVG is a very ominous sign, associated with a high risk of mortality, greater than 50% (Nelson et al. 2009), if other signs of necrotic bowel are present; such as abdominal pain. Medical conditions associated with HPVG include mesenteric ischemia, active peptic ulcer disease, intestinal obstruction and/or dilation, ulcerative colitis or Crohns disease. When stratifying the risk for patients, the clinical events initiating the HPVG are the most important factors in determining the patient’s prognosis. HPVG is most commonly associated with bowel necrosis (72%), ulcerative colitis (8%) intra abdominal abscesses (6%), small bowel obstruction (3%) and gastric ulcers (3%) (Liebman et al). All of these disease entities represent potentially lethal end results. This patient had a known history of hypertension and hypercholesterolemia, which together are risk factors for ischemic bowel, however the most important diagnostic piece of history for this patient was the intermittent cocaine use. Cocaine is a known alpha adrenergic stimulant. There are an abundance of alpha adrenergic receptors found in the vessel walls leading to a significantly reduced blood flow in local areas of the gut secondary to cocaine use. Cocaine also is a direct vasoconstrictor at the endothelial membrane, exerting its effects by promoting the release of endothelin-1 from the endothelial cells. (Schwartz et al) Other mechanisms leading to mesenteric ischemia caused by cocaine include decreased fibrinolysis activity increasing platelet aggregation and thrombus formation. (Wattoo et al). Mesenteric Ischemia may be caused by four different categories of pathology including Mesenteric Artery Thrombosis, Mesenteric Artery Embolus, Mesenteric Vein Thrombosis or Non occlusive Ischemia. Cocaine is included in the latter of the categories which also includes other inducers of low flow states such as sepsis, hypotensive states, digoxin, beta blockers etc. (Ofer et al). However the majority of these cases are found in patients during their hospitalization. The peculiar but dramatic change in the patient’s CT scans can be explained by intermittent cocaine induced vasospasm leading to mesenteric ischemia, which caused the transient HPVG. Physical Exam: Vitals T: 98.4 P: 110 BP: 160/94 RR: 22. Moderate distress, Alert and Oriented to person, time and place HEENT: Pupils equal/reactive, mucous membranes pink and moist Cardiac- Regular Rate and Rhythm 2/6 systolic ejection murmur Lungs- Clear to auscultation bilaterally Abdomen- Scars noted in the epigastric region, moderate diffuse tenderness to palpation. Bowel sounds present throughout. No distension. Neurologic-No focal neurologic deficits Cranial Nerves 2-12 intact. 5/5 muscle strength in Upper and Lower Extremities, 2+ Patellar reflexes Bilaterally Skin: Warm, mildly diaphoretic Figure 1.- Hepatic portal venous gas present (Hospital day 0 in the ED) ED/Hospital Course: The patient was found to be in moderate distress with his exam revealing diffuse abdominal pain out of proportion to his physical exam. Due to this exam finding and recent similar presentation with a normal work up, the patient was started on normal saline fluid bolus, morphine for pain and Pepcid. Abdominal labs and a CT without contrast of his abdomen and pelvis were ordered. After the patient returned from CT scan his mental status quickly began to deteriorate and the patient was intubated prior to transfer to the medical ICU. The CT scan in the Emergency Department displayed hepatic portal venous gas (HPVG). Surgery was consulted however before the surgical residents could evaluate the patient he was transferred to the MICU sedated and intubated. A second CT scan with IV contrast was preformed in the Medical ICU several hours later to better characterize the initial findings. On the second CT scan with contrast the HPVG previously seen was no longer present; the scan was found to have no acute pathology observed. The patient was extubated the next day and discharged on the third hospital day without needing surgery. He later admitted to inhaling large amounts of cocaine prior to both presentations of abdominal pain. References: Nelson, A. L., T. M. Millington, D. Sahani, R. T. Chung, C. Bauer, M. Hertl, A. L. Warshaw, and C. Conrad. "Hepatic Portal Venous Gas: The ABCs of Management." Archives of Surgery 144.6 (2009): 575-81. Print Liebman PR, Patten MT, Manny J, Benfield JR, Hechtman HB. Hepatic portal venous gas in adults: etiology, pathophysiology and clinical significance. Ann Surg. 1978;187:281–287. Wattoo,M..A , Osundeko O. “Cocaine-induced intestinal ischemia” West J Med 1999;170:47-49. Schwartz, B.G. Shereif R. “Contemporary Reviews in Cardiovascular Medicine.” Circulation. 2010. 122:2558-2569. Ofer A, Abadi S, Nitecki S, et al. “Multidetector CT angiography in the evaluation of acute mesenteric ischemia.”Eur Radiol 2009;19: 24-30. Figure 2.- No Hepatic Portal Venous gas present (Hospital Day 1)