Download
1 / 1
10 likes | 79 Views
Adherence to oral methadone: prevalence, correlates & implications for prescribers . Institute of Psychiatry at The Maudsley. M Haskew¹, J Dunn 2 , J Bearn 3 .

E N D
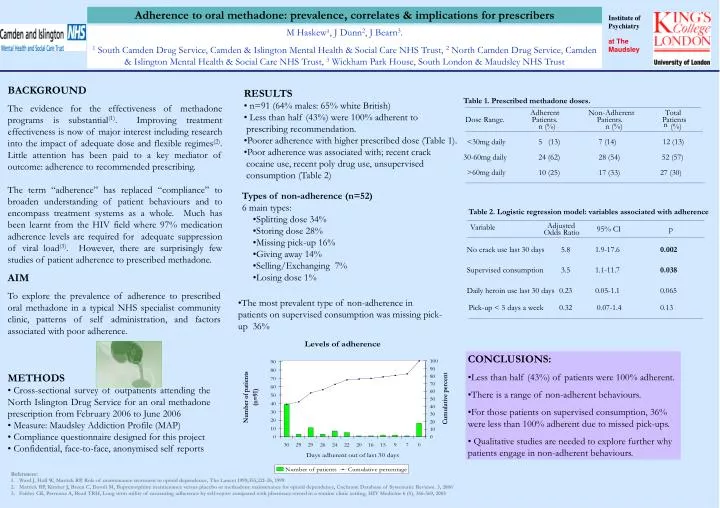
Adherence to oral methadone: prevalence, correlates & implications for prescribers Institute of Psychiatry at The Maudsley M Haskew¹, J Dunn2, J Bearn3. 1 South Camden Drug Service, Camden & Islington Mental Health & Social Care NHS Trust, 2 North Camden Drug Service, Camden & Islington Mental Health & Social Care NHS Trust, 3 Wickham Park House, South London & Maudsley NHS Trust • RESULTS • n=91 (64% males: 65% white British) • Less than half (43%) were 100% adherent to • prescribing recommendation. • Poorer adherence with higher prescribed dose (Table 1). • Poor adherence was associated with; recent crack • cocaine use, recent poly drug use, unsupervised • consumption (Table 2) BACKGROUND The evidence for the effectiveness of methadone programs is substantial(1). Improving treatment effectiveness is now of major interest including research into the impact of adequate dose and flexible regimes(2). Little attention has been paid to a key mediator of outcome: adherence to recommended prescribing. The term “adherence” has replaced “compliance” to broaden understanding of patient behaviours and to encompass treatment systems as a whole. Much has been learnt from the HIV field where 97% medication adherence levels are required for adequate suppression of viral load(3). However, there are surprisingly few studies of patient adherence to prescribed methadone. Table 1. Prescribed methadone doses. Adherent Non-Adherent Total Dose Range. Patients. Patients. Patients n n (%) n (%) (%) <30mg daily 5 (13) 7 (14) 12 (13) 30-60mg daily 28 (54) 52 (57) 24 (62) >60mg daily 17 (33) 27 (30) 10 (25) • Types of non-adherence (n=52) • 6 main types: • Splitting dose 34% • Storing dose 28% • Missing pick-up 16% • Giving away 14% • Selling/Exchanging 7% • Losing dose 1% Table 2. Logistic regression model: variables associated with adherence Adjusted Variable 95% CI p Odds Ratio No crack use last 30 days 5.8 1.9-17.6 0.002 Supervised consumption 3.5 1.1-11.7 0.038 AIM To explore the prevalence of adherence to prescribed oral methadone in a typical NHS specialist community clinic, patterns of self administration, and factors associated with poor adherence. Daily heroin use last 30 days 0.23 0.05-1.1 0.065 • The most prevalent type of non-adherence in patients on supervised consumption was missing pick-up 36% Pick-up < 5 days a week 0.32 0.07-1.4 0.13 • CONCLUSIONS: • Less than half (43%) of patients were 100% adherent. • There is a range of non-adherent behaviours. • For those patients on supervised consumption, 36% were less than 100% adherent due to missed pick-ups. • Qualitative studies are needed to explore further why patients engage in non-adherent behaviours. • METHODS • Cross-sectional survey of outpatients attending the North Islington Drug Service for an oral methadone prescription from February 2006 to June 2006 • Measure: Maudsley Addiction Profile (MAP) • Compliance questionnaire designed for this project • Confidential, face-to-face, anonymised self reports • References: • Ward J, Hall W, Mattick RP, Role of maintenance treatment in opioid dependence, The Lancet 1999;353,221-26, 1999. • Mattick RP, Kimber J, Breen C, Davoli M, Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence, Cochrane Database of Systematic Reviews. 3, 2006 • 3. Fairley CK, Permana A, Read TRH, Long term utility of measuring adherence by self-report compared with pharmacy record in a routine clinic setting, HIV Medicine 6 (5), 366-369, 2005