Download

1 / 11
110 likes | 191 Views
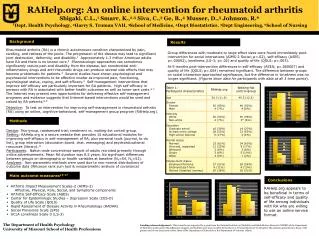
School of Health Professions Education Prof. dr. Albert Scherpbier. The combination of virtual patients and small group discussions to promote reflective practice. Bas de Leng, PhD ICVP London, 26 April 2010. Risks of life…. Medical errors. Diagnostic errors: 5-15% of medical diagnosis

E N D
School of Health Professions Education Prof. dr. Albert Scherpbier The combination of virtual patients and small group discussions to promote reflective practice Bas de Leng, PhD ICVP London, 26 April 2010
Medical errors • Diagnostic errors: 5-15% of medical diagnosis • Taxonomy of diagnostic error (Graber,2005): • No-fault errors • System-related errors • Cognitive errors • Cognitive errors contributeto 75% of all diagnostic errrors • ‘Premature closure’ mostcommon cognitive error
Education to prevent cognitive errors Relationships between reliability and effort of diagnostic decision making (Graber, 2009) ideas for educational approaches More Deductive reasoning Monitoring, reflection Pre-expert reasoning: heuristics Effort Expert thinking Expert thinking Less Low High Accuracy
Increase expertise • Deliberate practice with coaching and feedback by more accomplished professionals (Ericsson, 2003) • Access to a large numbers of patients with similar symptoms for which the correct diagnosis is validated • Virtual patients can supplement real patient encounters
Learn to apply reflective thinking Learning to: • Recognize and understand the most likely diagnostic pitfalls (Croskerry, 2003) • Use a checklist for the diagnostic process including ‘reflection’.
Clinical reasoning sessions Ingredients: Virtual patients based on real cases in which ‘premature closure’ had occurred Procedure to induce reflective diagnostic reasoning (Mamede, 2008)
Clinical reasoning sessions • Procedure: • All residents simultaneously worked out the same virtual patient • And the end of the work-up they had a moderated discussion on their clinical reasoning • The logged actions and their notes were starting points for the discussion
Evaluation of perceptions Two student questionnaires: Experiences with the use virtual patients. With 12 statements on: Authenticity Professional approach Coaching Learning effect Overall judgment Experiences with the integration of virtual patients. With 20 statements on: Teaching presence Cognitive presence Social presence Learning effect Overall judgment
Conclusion Residents perceived a session combining individual virtual patient workup with small group discussions as a valuable learning activity for clinical reasoning. The clinical supervisor found the presented teaching approach feasible for the medical specialist training at the workplace.
Future research Evaluation of clinical reasoning sessions with VPs on 3rd and 4th level of Kirkpatrick: Do they learn clinical reasoning and reflective practice from this activity? Do the learning outcomes transfer to clinics and wards?