Download
1 / 1
10 likes | 192 Views
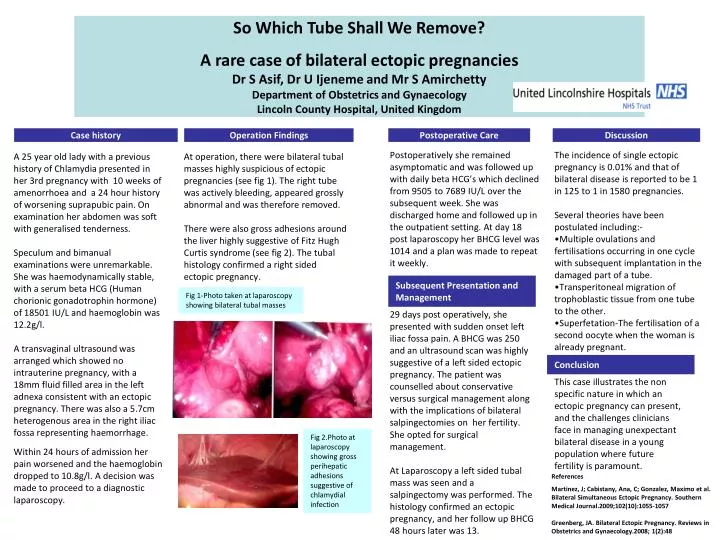
So Which Tube Shall We Remove? A rare case of bilateral ectopic pregnancies Dr S Asif, Dr U Ijeneme and Mr S Amirchetty Department of Obstetrics and Gynaecology Lincoln County Hospital, United Kingdom. Case history. Operation Findings. Postoperative Care. Discussion.

E N D
So Which Tube Shall We Remove? A rare case of bilateral ectopic pregnancies Dr S Asif, Dr U Ijeneme and Mr S Amirchetty Department of Obstetrics and Gynaecology Lincoln County Hospital, United Kingdom Case history Operation Findings Postoperative Care Discussion A 25 year old lady with a previous history of Chlamydia presented in her 3rd pregnancy with 10 weeks of amenorrhoea and a 24 hour history of worsening suprapubic pain. On examination her abdomen was soft with generalised tenderness. Speculum and bimanual examinations were unremarkable. She was haemodynamically stable, with a serum beta HCG (Human chorionic gonadotrophin hormone) of 18501 IU/L and haemoglobin was 12.2g/l. A transvaginal ultrasound was arranged which showed no intrauterine pregnancy, with a 18mm fluid filled area in the left adnexa consistent with an ectopic pregnancy. There was also a 5.7cm heterogenous area in the right iliac fossa representing haemorrhage. Within 24 hours of admission her pain worsened and the haemoglobin dropped to 10.8g/l. A decision was made to proceed to a diagnostic laparoscopy. At operation, there were bilateral tubal masses highly suspicious of ectopic pregnancies (see fig 1). The right tube was actively bleeding, appeared grossly abnormal and was therefore removed. There were also gross adhesions around the liver highly suggestive of Fitz Hugh Curtis syndrome (see fig 2). The tubal histology confirmed a right sided ectopic pregnancy. Postoperatively she remained asymptomatic and was followed up with daily beta HCG’s which declined from 9505 to 7689 IU/L over the subsequent week. She was discharged home and followed up in the outpatient setting. At day 18 post laparoscopy her BHCG level was 1014 and a plan was made to repeat it weekly. • The incidence of single ectopic pregnancy is 0.01% and that of bilateral disease is reported to be 1 in 125 to 1 in 1580 pregnancies. • Several theories have been postulated including:- • Multiple ovulations and fertilisations occurring in one cycle with subsequent implantation in the damaged part of a tube. • Transperitoneal migration of trophoblastic tissue from one tube to the other. • Superfetation-The fertilisation of a second oocyte when the woman is already pregnant. Subsequent Presentation and Management Fig 1-Photo taken at laparoscopy showing bilateral tubal masses 29 days post operatively, she presented with sudden onset left iliac fossa pain. A BHCG was 250 and an ultrasound scan was highly suggestive of a left sided ectopic pregnancy. The patient was counselled about conservative versus surgical management along with the implications of bilateral salpingectomies on her fertility. She opted for surgical management. At Laparoscopy a left sided tubal mass was seen and a salpingectomy was performed. The histology confirmed an ectopic pregnancy, and her follow up BHCG 48 hours later was 13. Conclusion This case illustrates the non specific nature in which an ectopic pregnancy can present, and the challenges clinicians face in managing unexpectant bilateral disease in a young population where future fertility is paramount. Fig 2.Photo at laparoscopy showing gross perihepatic adhesions suggestive of chlamydial infection References Martinez, J; Cabistany, Ana, C; Gonzalez, Maximo et al. Bilateral Simultaneous Ectopic Pregnancy. Southern Medical Journal.2009;102(10):1055-1057 Greenberg, JA. Bilateral Ectopic Pregnancy. Reviews in Obstetrics and Gynaecology.2008; 1(2):48