Download
1 / 53
730 likes | 1.23k Views
CONSERVATIVE TREATMENT OF FRACTURES. Dr. Muhammad ASIF Orthopedic Surgeon Department of Orthopaedics College of Medicine King Khalid University Hospital. Fracture management.

E N D
CONSERVATIVE TREATMENT OF FRACTURES Dr. Muhammad ASIF Orthopedic Surgeon Department of Orthopaedics College of Medicine King Khalid University Hospital
Fracture management • The ideal goal of fracture management is anatomical reduction and function restoration compatible with the severity of injury, age, occupation and activity of daily living of injured patient. • Either • Operative • Non operative (Conservative) • Traction • Splint (Cast / Slab)
Traction • Tractionis the application of a pulling force to a part of the body • Purpose: • to reduce, align, and immobilize fractures; • Unstable and unfixable • When reduction and/or proper length cannot be maintained by static immobilization • to minimize muscle spasm • to prevent or reduce skeletal deformities or muscle contractures.
Classification of Traction • Skin Traction : is maintained by direct application of a pulling force on the patient’s skin . Generally temporary measure. • To reduce muscle spasms • To maintain immobilization before surgery • In children • Skeletal Traction : applied to bone by means of a pin or wire surgically inserted into the bone, • providing a strong steady, continuous pull, and • can be used for prolonged periods .
Complications of traction • Neurovascular compromise. • Inadequate fracture alignment.. • Skin breakdown . • Soft tissue injury • Pin tract infection . • Osteomyelitis can occur with skeletal traction.
Complications of traction • complications from immobility especially with long term traction and in elder pt. • Pressure ulcer • Pneumonia • Constipation • Anorexia • Urinary stasis and infection • Venous stasis with DVT
General Indications for CAST 1. Most fractures in children: a. Tremendous capacity of remodeling. b. Non union and stiffness is unlikely. 2. Undisplaced fracture 3. Poor bone Quality: Osteoporosis. 4. Unfixable fracture e.g. severe comminuted. 5. Systemic contraindication. 6. Local contraindication. 7. Psychosocial problem.
Splint / Cast • Principle: • To stabilize joint above and joint below the site of injury whenever and wherever is possible • Objectives: • To hold broken bone anatomically to prevent malunion. • To reduce excessive movements to prevent non union. • To get early function
How to Preserve Function? • Immobilize only joint necessary, • Range of motion of uninvolved joints. • Isometric exercise. • Physiotherapy after cast removal. • Weight bearing whenever possible in case of lower limb fracture.
What are casts made of ? • The outside, or hard part of the cast, two different kinds of casting materials. • Plaster (POP) - white in color. hemihydrated calcium sulphate. On adding water it solidifies by an exothermic reaction into hydrated calcium sulphate • fiberglass - variety of colors, patterns, and designs. • inside of the cast Cotton and other synthetic materials are used to line theinside of the cast to make it soft and to provide padding around bony areas.
Plaster is usually used in the early stages of treatment, • Displaced Fracture that need manipulation • can be molded more precisely. • heavy • must remain dry, water will distort the cast • Fiberglass • Can be used in UndisplacedFx if swelling not expected • healing process has already started. • lighter weight, durable, require less maintenance.
Closed Reduction Method • Adequate analgesia / anaesthesia • Traction – countertraction • Increase the deformity if needed, to reduce / lock on fragments • Correct rotational deformity as well. • Remove any rings from fingers or affected limbs • All acute injuries (<48 hours post injury) fully padded well molded plaster, full casts may be splittted.
After Closed Reduction and Casting • must have circulation check • Plaster takes 48 hours to become fully dry and harden so take care. • Weekly radiographs for 3 weeks to confirm acceptable reduction. • Can re-manipulate within 3 weeks after injury if displaced.
Colles’ Fracture • Displaced dorsolaterrally • Treatment: Cast +/- surgery, depending on shortening and displacement
Scaphoid Bone FX • Retrograde blood supply • Total healing time of 10-12 weeks or more
Boxer’s Fracture • Classically neck of the fifth metacarpal • bump over the back of palm just below the small finger knuckle • Treatment: casting or surgery (pins)
Patellar Fracture • Fall onto kneecap or when quadriceps is contracting • Attempt “straight leg raise” If Extensor mechanism intact / undisplacedFx Cast / Slab
Fracture of 5th Metatarsal • Avulsion Fracture • base of 5th metatarsal from pull of attached tendon; • heal well in cast • Jones Fracture • Transverse fracture through base of 5th metatarsal, about 1-2 cm from tip; • cast for 6-8 wks if undisplaced
Torus Fracture • “Buckle fracture” • mostly in children; metaphysis • cast for 2-4 weeks
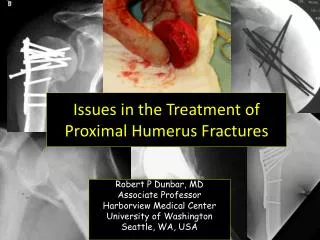
Type 1 S/C Fxhumerus:non-displaced conservative • Note the non- displaced fracture (Red Arrow) • Note the posterior fat pad (Yellow Arrows)
Type 2: Angulated/displaced fracture with intact posterior cortex; close reduction and K-wires fixation
Type 3: Complete displacement, with no contact between fragments; close / open reduction and K-Wire fixation
Post Cast instructions • Keep your limb elevated to prevent swelling. • Apply an ice bag to injured area. • Keep the cast clean and dry. • Check for cracks or breaks in the cast. • Rough edges should be padded to protect the skin from scratches. • Do not scratch the skin under the cast by inserting sticks. • Encourage patient to move his/her fingers or toes to promote circulation
Contd • Prevent small toys or objects from being put inside the cast. • Do not put powders or lotion inside the cast. • Cover the cast while your child is eating to prevent food spills and crumbs from entering the cast. • Do not use the abduction bar on the cast to lift or carry the child. • Use a diaper or sanitary napkin around the genital area to prevent leakage or splashing of urine.
How To Know if Something Is Wrong With Your Cast • Pain that is not adequately controlled with medication prescribed by your doctor. • Increasing swelling • Numbness or tingling in the extremity (hand or foot). • Inability to move your fingers or toes beyond the cast. • Circulation problems in your hand or foot. • Loosening, splitting or breaking of the cast. • Unusual odors, sensations, or wounds beneath the cast. • If you develop a fever or generalized illness
Complications of cast • Compartment syndrome, tight cast that restricts swelling. • Impaired distal neurovascular. • most serious is deep venous thrombosis leading to pulmonary embolism----calf pain. • Re displacement of fracture. • stiff joints, muscle wasting. • Plaster Sores. • Malunion, Nonunion, Delayed union
Cast Burns- can occur during cast removal if blade dull or improper technique used.