Download
1 / 1
10 likes | 98 Views
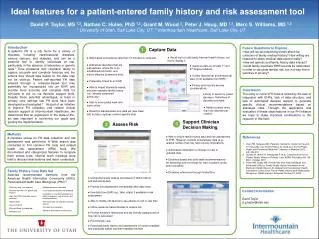
Capture Data. 1. Support Clinician Decision Making. 3. Assess Risk. 2. Family History Core Data Set Selected recommended elements from the American Health Information Community (AHIC) Personalized Health Care Workgroup (PHC) 3 :. Relative name (first and last)

E N D
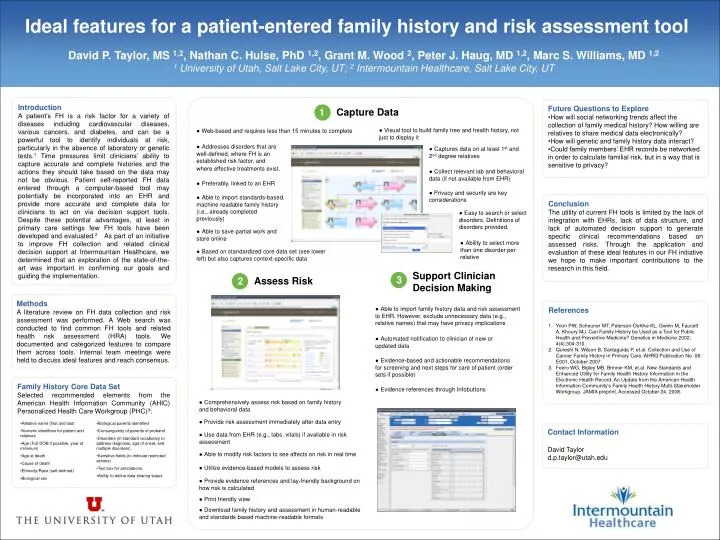
Capture Data 1 Support Clinician Decision Making 3 Assess Risk 2 Family History Core Data Set Selected recommended elements from the American Health Information Community (AHIC) Personalized Health Care Workgroup (PHC)3: • Relative name (first and last) • Numeric identifiers for patient and relatives • Age (Full DOB if possible, year at minimum) • Age at death • Cause of death • Ethnicity/Race (self-defined) • Biological sex • Biological parents identified • Consanguinity of parents of proband • Disorders (in standard vocabulary to address diagnosis, age of onset, and multiple disorders) • Sensitive fields (to indicate restricted access) • Text box for annotations • Ability to define data sharing status Ideal features for a patient-entered family history and risk assessment tool • David P. Taylor, MS 1,2, Nathan C. Hulse, PhD 1,2, Grant M. Wood 2, Peter J. Haug, MD 1,2, Marc S. Williams, MD 1,2 • 1 University of Utah, Salt Lake City, UT; 2 Intermountain Healthcare, Salt Lake City, UT Introduction A patient’s FH is a risk factor for a variety of diseases including cardiovascular diseases, various cancers, and diabetes, and can be a powerful tool to identify individuals at risk, particularly in the absence of laboratory or genetic tests.1 Time pressures limit clinicians’ ability to capture accurate and complete histories and the actions they should take based on the data may not be obvious. Patient self-reported FH data entered through a computer-based tool may potentially be incorporated into an EHR and provide more accurate and complete data for clinicians to act on via decision support tools. Despite these potential advantages, at least in primary care settings few FH tools have been developed and evaluated.2 As part of an initiative to improve FH collection and related clinical decision support at Intermountain Healthcare, we determined that an exploration of the state-of-the-art was important in confirming our goals and guiding the implementation. • Future Questions to Explore • How will social networking trends affect the collection of family medical history? How willing are relatives to share medical data electronically? • How will genetic and family history data interact? • Could family members’ EHR records be networked in order to calculate familial risk, but in a way that is sensitive to privacy? ●Visual tool to build family tree and health history, not just to display it ● Web-based and requires less than 15 minutes to complete ●Addresses disorders that are well-defined, where FH is an established risk factor, and where effective treatments exist. ●Captures data on at least 1st and 2nd degree relatives ●Collect relevant lab and behavioral data (if not available from EHR) ●Preferably, linked to an EHR ● Privacy and security are key considerations ●Able to import standards-based, machine readable family history (i.e., already completed previously) Conclusion The utility of current FH tools is limited by the lack of integration with EHRs, lack of data structure, and lack of automated decision support to generate specific clinical recommendations based on assessed risks. Through the application and evaluation of these ideal features in our FH initiative we hope to make important contributions to the research in this field. ●Easy to search or select disorders. Definitions of disorders provided. ●Able to save partial work and store online ●Ability to select more than one disorder per relative ●Based on standardized core data set (see lower left) but also captures context-specific data Methods A literature review on FH data collection and risk assessment was performed. A Web search was conducted to find common FH tools and related health risk assessment (HRA) tools. We documented and categorized features to compare them across tools. Internal team meetings were held to discuss ideal features and reach consensus. • References • Yoon PW, Scheuner MT, Peterson-Oehlke KL, Gwinn M, Faucett A, Khoury MJ. Can Family History be Used as a Tool for Public Health and Preventive Medicine? Genetics in Medicine 2002; 4(4):304-310. • Qureshi N, Wilson B, Santaguida P, et.al. Collection and Use of Cancer Family History in Primary Care. AHRQ Publication No. 08-E001, October 2007. • Feero WG, Bigley MB, Brinner KM, et.al. New Standards and Enhanced Utility for Family Health History Information in the Electronic Health Record: An Update from the American Health Information Community's Family Health History Multi-Stakeholder Workgroup. JAMIA preprint, Accessed October 24, 2008. ●Able to import family history data and risk assessment to EHR. However, exclude unnecessary data (e.g., relative names) that may have privacy implications ●Automated notification to clinician of new or updated data ●Evidence-based and actionable recommendations for screening and next steps for care of patient (order sets if possible) ●Evidence references through Infobuttons ●Comprehensively assess risk based on family history and behavioral data ● Provide risk assessment immediately after data entry Contact Information David Taylor d.p.taylor@utah.edu ●Use data from EHR (e.g., labs, vitals) if available in risk assessment ●Able to modify risk factors to see affects on risk in real time ●Utilize evidence-based models to assess risk ●Provide evidence references and lay-friendly background on how risk is calculated ●Print friendly view ●Download family history and assessment in human-readable and standards based machine-readable formats