Download
1 / 1
10 likes | 88 Views
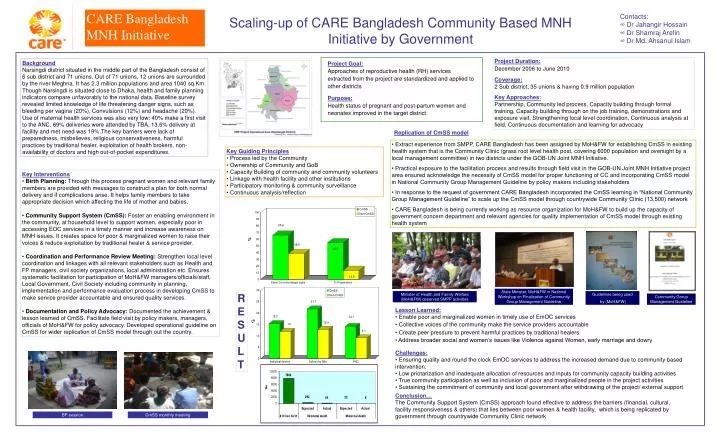
%. %. State Minister, MoH&FW in National Workshop on Finalization of Community Group Management Guideline. Minister of Health and Family Welfare (MoH&FW) observed SMPP activities. Guidelines being used by (MoH&FW). RESULT. Community Group Management Guideline. BP session.

E N D
% % State Minister, MoH&FW in National Workshop on Finalization of Community Group Management Guideline Minister of Health and Family Welfare (MoH&FW) observed SMPP activities Guidelines being used by (MoH&FW) RESULT Community Group Management Guideline BP session CmSS monthly meeting CARE Bangladesh MNH Initiative • Contacts: • Dr Jahangir Hossain • Dr Shamraj Arefin • Dr Md. Ahsanul Islam Scaling-up of CARE Bangladesh Community Based MNH Initiative by Government Project Duration: December 2006 to June 2010 Coverage: 2 Sub district, 35 unions & having 0.9 million population Key Approaches: Partnership, Community led process, Capacity building through formal training, Capacity building through on the job training, demonstrations and exposure visit, Strengthening local level coordination, Continuous analysis at field, Continuous documentation and learning for advocacy Background Narsingdi district situated in the middle part of the Bangladesh consist of 6 sub district and 71 unions. Out of 71 unions, 12 unions are surrounded by the river Meghna. It has 2.3 million populations and area 1040 sq.Km. Though Narsingdi is situated close to Dhaka, health and family planning indicators compare unfavorably to the national data. Baseline survey revealed limited knowledge of life threatening danger signs, such as bleeding per vagina (20%), Convulsions (12%) and headache (20%). Use of maternal health services was also very low: 40% make a first visit to the ANC, 69% deliveries were attended by TBA, 13.6% delivery at facility and met need was 19%.The key barriers were lack of preparedness, misbelieves, religious conservativeness, harmful practices by traditional healer, exploitation of health brokers, non-availability of doctors and high out-of-pocket expenditures. Project Goal: Approaches of reproductive health (RH) services extracted from the project are standardized and applied to other districts Purpose: Health status of pregnant and post-partum women and neonates improved in the target district Replication of CmSS model • Extract experience from SMPP, CARE Bangladesh has been assigned by MoH&FW for establishing CmSS in existing health system that is the Community Clinic (grass root level health post, covering 6000 population and oversight by a local management committee) in two districts under the GOB-UN Joint MNH Initiative. • Practical exposure to the facilitation process and results through field visit in the GOB-UN Joint MNH Initiative project area ensured acknowledge the necessity of CmSS model for proper functioning of CC and incorporating CmSS model in National Community Group Management Guideline by policy makers including stakeholders • In response to the request of government CARE Bangladesh incorporated the CmSS learning in “National Community Group Management Guideline” to scale up the CmSS model through countrywide Community Clinic (13,500) network • CARE Bangladesh is being currently working asresource organization for MoH&FW to build up the capacity of government concern department and relevant agencies for quality implementation of CmSS model through existing health system • Key Guiding Principles • Process led by the Community • Ownership of Community and GoB • Capacity Building of community and community volunteers • Linkage with health facility and other institutions • Participatory monitoring & community surveillance • Continuous analysis/reflection • Key Interventions • Birth Planning: Through this process pregnant women and relevant family members are provided with messages to construct a plan for both normal delivery and if complications arise. It helps family members to take appropriate decision which affecting the life of mother and babies. • Community Support System (CmSS): Foster an enabling environment in the community, at household level to support women, especially poor in accessing EOC services in a timely manner and increase awareness on MNH issues. It creates space for poor & marginalized women to raise their voices & reduce exploitation by traditional healer & service provider. • Coordination and Performance Review Meeting: Strengthen local level coordination and linkages with all relevant stakeholders such as Health and FP managers, civil society organizations, local administration etc. Ensures systematic facilitation for participation of MoH&FW managers/officials/staff, Local Government, Civil Society including community in planning, implementation and performance evaluation process in developing CmSS to make service provider accountable and ensured quality services. • Documentation and Policy Advocacy: Documented the achievement & lesson learned of CmSS. Facilitate field visit by policy makers, managers, officials of MoH&FW for policy advocacy. Developed operational guideline on CmSS for wider replication of CmSS model through out the country. Lesson Learned: • Enable poor and marginalized women in timely use of EmOC services • Collective voices of the community make the service providers accountable • Create peer pressure to prevent harmful practices by traditional healers • Address broader social and women’s issues like Violence against Women, early marriage and dowry Challenges: • Ensuring quality and round the clock EmOC services to address the increased demand due to community based intervention. • Low priotarization and inadequate allocation of resources and inputs for community capacity building activities • True community participation as well as inclusion of poor and marginalized people in the project activities • Sustaining the commitment of community and local government after withdrawing of the project/ external support Conclusion… The Community Support System (CmSS) approach found effective to address the barriers (financial, cultural, facility responsiveness & others) that lies between poor women & health facility, which is being replicated by government through countrywide Community Clinic network