Download
1 / 34
360 likes | 592 Views
The olfactory System and limbic system. Idara C. Eshiet. The olfactory system ( CN1). Introduction. The sense of smell is much less essential than vision, audition or the somatic senses but olfactory dysfunction is considered and important diagnostic sign and will be therefore reviewed.

E N D
The olfactory System and limbic system Idara C. Eshiet
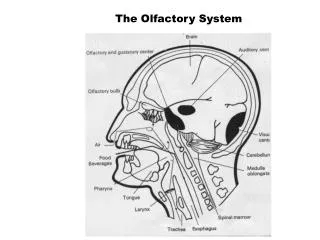
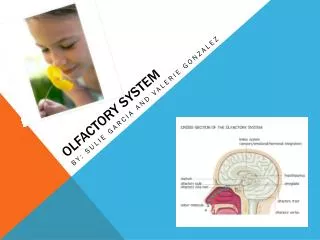
Introduction The sense of smell is much less essential than vision, audition or the somatic senses but olfactory dysfunction is considered and important diagnostic sign and will be therefore reviewed. The sense of smell and taste are intimately related and are therefore classified as Special Visceral Afferent (SVA). It is the only sensation that is transmitted directly to the cortex without relay in the Thalamus. Olfactory cells are also regularly replaced from precursor cells. The olfactory nerve ( CN 1) is composed of unmyelinated axons of receptor cells located in the olfactory mucosa in the nasal cavity.
The first order neuron in the olfactory pathway is also the sensory receptor. The olfactory receptor cells are scattered among supporting cells. Each receptor cell consists of a small bipolar nerve cell with a coarse peripheral process that pass to the surface of the membrane and a fine central process. From the peripheral processes a number of short cilia arise , the olfactory hairs which project into the mucus covering the the surface of the mucus membrane. Odorants bind to receptor proteins on the cilia.
The fine central processes form the olfactory nerve fibers . Bundles of these fibers pass through foramina in the cribiform plate of ethmoid to constitute 20 olfactory fila on each side. Most of the fibers terminate on mitral cells in the olfactory bulb. The nerve fibers form a synaptic connection with the dendrites of the mitral cells called Glomeruli. Smaller cells called granule and periglomerularcells synapse also with the mitral cells ( Inhibitory).
Olfactory tract The relay from the mitral cells constitute the olfactory tract. It runs from the posterior end of the olfactory bulb beneath the inferior surface of the frontal lobe of the brain. As it reaches the anterior perforated substance, it divides into medial and lateral olfactory striae. The lateral olfactory striaecarries axons to the olfactory areas of the cerebral cortex namely, the parts of the orbital surface of the frontal lobe,as well as the uncus, entorhinal area and medial amygdaloid nucleus of the temporal lobe. The medial olfactory striaecarries the fibers that cross the median plane in the anterior commissure to pass to the olfactory bulb of the opposite side.
Olfactory Connections Olfactory connections are said to reach numerous structures including the Hippocampus, regions in the reticular formation including the Salivatory nuclei, Dorsal motor nucleus of Vagus, Dorsomedial nucleus of the thalamus, medial amygdaloid nucleus. Through these complex interactions, the sense of smell influences visceral functions( salivation, gastric secretions, peristalsis), social interaction and reproductive behavior. Some of the pathways involved in transmitting olfaction include the medial forebrain bundle ( hypothalamus), striaemedullaris thalami ( to dorso medial nucleus), Striaeterminalis ( from amygdala), Dorsal longitudinal fasciculus ( from hypothalamus to brain stem visceral centers)
The Uncus It is of clinical significance because: • Seizures often originate in this area ( uncinate fits). These seizures are often preceded by hallucinations of disagreeable odors. • When the volume of the temporal lobe is increased due to tumors, hemorrhage or edema, the uncus can press against the brainstem and cranial nerves with serious consequences( Uncalherniation). The herniatinguncus and adjacent part of the parahippocampalgyrus push the brainstem to the opposite side, resulting in damage by pressure against the taut free margin of the tentoriumcerebelli. • The brainstem damage is usually contralateral to the side of the herniation.
Anosmia Loss of smell is term Anosmia. It is usually bilateral caused by common cold or allergic rhinitis. Unilateral anosmia could result from disease affecting the olfactory nerve, bulb or tract. A unlateral lesion can’t produce complete anosmia because of the bilaterality of the olfactory pathway. Fractures of the cribiform plate of ethmoid cause avulsion of the olfactory nerves. Cerebral tumors can produce anosmia by pressing on the olfactory bulb or tract.
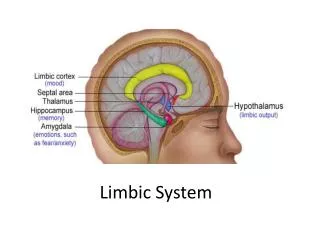
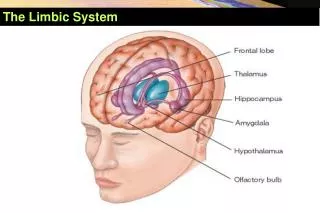
Introduction Limbic is a Latin term which means border. Like the familiar word “limbo”, it means an intermediate or transitional state, which is a border. In this case, the border is between the neocortex and the subcortical structures (diencephalon). The limbic system includes the hippocampal formation, amygdala, septal nuclei, cingulate cortex, entorhinal cortex, perirhinal cortex, and parahippocampal cortex. These last three cortical areas comprise different portions of the temporal lobe. (Some experts would also include parts of the hypothalamus, thalamus, midbrain reticular formation, and olfactory areas in the limbic system.) These structures are sometimes called the Papez circuit after the neuroanatomist that pointed out their interconnections.
The Hippocampus This is a phylogenetically old part of the cerebral cortex located within the temporal lobe. It typically refers to the dentate gyrus, the hippocampus proper (i.e., cornuammonis), and the subicular cortex. A hippocampal formation is located in the temporal lobe of each cerebral cortex, medial to the inferior horn of the lateral ventricle. Hippocampus means seahorse in Greek. Each hippocampus looks like a seahorse due to the way it is folded during development.
The hippocampus projects by way of the fornix to the mammillary bodies of the hypothalamus and septal nuclei. The fornix is a large fiber bundle that follows a C-shaped course from the hippocampus to its target areas . The fibers destined for the fornix collect on the surface of the Hippocampus as a thin sheet that converges into a bundle of fibers called the Fimbria. The fimbria leaves the posterior end of the hippocampus forming the Crus of the fornix. The two crura from both sides join together forming the Body of fornix that heads to the mammillary bodies in the Hypothalamus.
Lesions of the Hippocampus People with lesions of the temporal lobe including the Hippocampus can have a disruption of memory. This deficit is observed only when the damage is bilateral. It can be sometimes noticed with unilateral lesions. This deficit is a loss of Recent memories. This means that memory of recent events is lost. This is termed Anterograde Amnesia. A common cause of bilateral Hippocampal damage is anoxia from interruption of blood or oxygen supply. The Hippocampus is one of the first sites to be irreversibly damaged by transient ischemia or anoxia.
Korsakoff Syndrome Patient with this syndrome also present with Anterograde amnesia. Patients could also present with retrograde amnesia and confabulate( make up stories) to make up for past memories. It is mainly seen in alcoholics who have thymine deficiency and follows an acute presentation of Wernicke’sEncephalopathy. Wernicke’s Encephalopathy presents with Ocular palsies, confusion and gait ataxia. It is also related to Thymine deficiency. In Wernicke- korsakoff Syndrome, lesion are always found in the mammillary bodies and the Dorsomedial nucleus of the Thalamus.
Amygdala This is a large nuclear complex located immediately rostral to the Hippocampus, within the temporal lobe. It is almond shaped. It is divided into different nuclei. It is usually seen as part of the Basal ganglia. It is involved in emotional expession and visceral functions. The amygdala receives inputs from all senses as well as visceral inputs. Since the amygdala is very important in emotional learning it is not surprising that visceral inputs are a major input source.
Function • Control of emotions • Control of sexual behavior • Control of food and water intake. The mechanisms for mediating these behavioral patterns are not well understood.
Afferents to the amygdala Visceral inputs come from the hypothalamus, septal area, orbital cortex. Olfactory sensory information comes from the olfactory bulb. Auditory, visual and somatosensory information comes from the temporal and anterior cingulate cortices.
Efferents from the Amygdala • Ventral amygdalofugal pathway – projects to the olfactory nucleus , anterior perforated substance, piriform cortex and ventral striatum( parts of the caudate, putamen and nucleus accumbenssepti). The ventral amygdalofugal pathway is important because it is a link whereby motivation and drives, through the limbic system, can influence responses. It is also a link whereby responses are learned. In this case, this is the link whereby associative learning takes place.
2. Striaterminalis to the Hypothalamus The striaterminalis overlaps with the ventral amygdalofugal pathway in that it also connects to the septal nuclei and hypothalamus and thus forms a loop. 3. Connects directly to the hippocampus 4. Directly to the entorhinal cortex 5. Directly to the dorsomedial nucleus of the thalamus
Kluver- Bucy Syndrome Bilateral damage to the rostro- ventral portion of the temporal lobes that includes the hippocampal formation, amygdala can lead to this syndrome. • Patients become Docile- previously violent patients displayed little or no emotion. • Anterograde amnesia • Hyperphagia • Hyperorality • Hypersexuality • Visual Agnosia- patients do not recognize complex visual patterns • Psychic blindness- Objects in the visual vield are treated inappropriately.
Septal Area It is a component of the limbic system located anterior to the hypothalamus. It consists of the Septal nucleus, the septum pellucidum, the small portion of the neocortex that forms part of the limbic lobe. Because of it’s connections with the hippocampus and hypothalamus it is considered as part of the limbic system. The hippocampus sends connections to the septal nuclei(area) by way of the columns of fornix. Its function is not well understood.
CingulateGyrus Is the portion of the limbic lobe that overlies the corpus callosum. It receives connections from the anterior nucleus of the thalamus. This puts it in close communication with the hypothalamus by way of the mammillothalamic tract. The cingulategyrus is connected to the parahipocampalgyrus by way of the cingulum. It is believed to be involved in the generation of emotional and visceral responses but it is not quite clear how.
Q1. Fiber bundles of the limbic system includes • Fornix • Mammillothalamic tract • Striaterminalis • Cingulum • All of the above
Q2. Kluver – bucy syndrome results due to • Unilateral temporal lobe damage • Bilateral temporal lobe damage • Damage to the cingulate cortex • Damage to the mammillary bodies