Download
1 / 8
80 likes | 289 Views
QUEST-2 Study : SMV + PEG-IFN + RBV for genotype 1. Design. Randomisation* 2 : 1 Double blind. W12. W24. W48. open-label. > 18 years Chronic HCV infection Genotype 1 Treatment-naïve HCV RNA > 10,000 IU /ml No HBV or HIV co-infection. SMV + PEG-IFN + RBV. PEG-IFN + RBV.

E N D
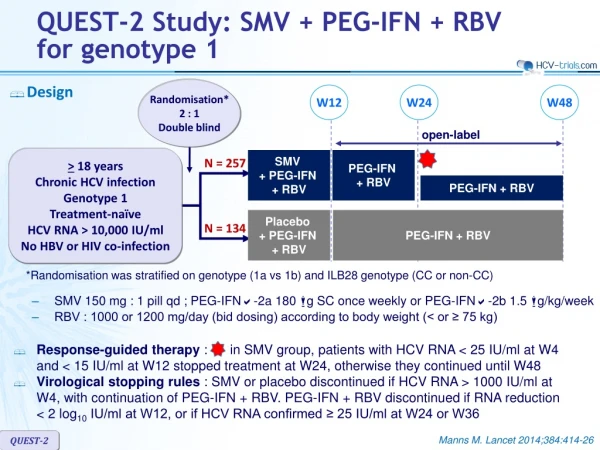
QUEST-2 Study: SMV + PEG-IFN + RBV for genotype 1 • Design Randomisation* 2 : 1 Double blind W12 W24 W48 open-label > 18 years Chronic HCV infection Genotype 1 Treatment-naïve HCV RNA > 10,000 IU/ml No HBV or HIV co-infection SMV + PEG-IFN + RBV PEG-IFN + RBV N = 257 PEG-IFN + RBV Placebo + PEG-IFN + RBV PEG-IFN + RBV N = 134 *Randomisation was stratified on genotype (1a vs 1b) and ILB28 genotype (CC or non-CC) • SMV 150 mg : 1 pill qd; PEG-IFNa-2a 180 mg SC once weekly or PEG-IFNa-2b 1.5 mg/kg/week • RBV : 1000 or 1200 mg/day (bid dosing) according to body weight (< or ≥ 75 kg) • Response-guided therapy : in SMV group, patients with HCV RNA < 25 IU/ml at W4 and < 15 IU/ml at W12 stopped treatment at W24, otherwise they continued until W48 • Virological stopping rules : SMV or placebo discontinued if HCV RNA > 1000 IU/ml at W4, with continuation of PEG-IFN + RBV. PEG-IFN + RBV discontinued if RNA reduction < 2 log10 IU/ml at W12, or if HCV RNA confirmed ≥ 25 IU/ml at W24 or W36 Manns M. Lancet 2014;384:414-26 QUEST-2
QUEST-2 Study: SMV + PEG-IFN + RBV for genotype 1 • Objectives • Difference in SVR12 (HCV RNA < 25 IU/ml) between the 2 groups : estimation of 45% in the control group, power of 90% to detect a difference > 20%, by intention to treat • Sensitivity analysis : comparison of SVR12 in both groups with a logistic regression model including baseline HCV RNA (log10 IU/ml, included as a continuous variable) and the stratification factors (HCV genotype 1 subtype and IL28B genotype) • Secondary endpoints : SVR24, % patients stopping treatment at W24 based on response-guided therapy, failure, safety • PEG-IFN Therapy • 63% of patients in each arm were randomized to receive PEG-IFN alfa-2a or PEG-IFN alfa-2b; the remainder was assigned PEG-IFN alfa-2a Manns M. Lancet 2014;384:414-26 QUEST-2
QUEST-2 Study: SMV + PEG-IFN + RBV for genotype 1 Baseline characteristics and patient disposition Manns M. Lancet 2014;384:414-26 QUEST-2
QUEST-2 Study: SMV + PEG-IFN + RBV for genotype 1 SVR12 (HCV RNA < 25 IU/ml) SMV Placebo % p < 0.0001 p < 0.0001 p < 0.0001 p < 0.0001 p= 0.25 100 82 81 82 80 75 75 53 50 50 46 43 50 25 N 257 134 107 57 24 14 79 40 150 77 0 All 1a All 1a Q80K+ 1a Q80K- 1b • Responseguidedtherapy (RGT) : in SMV group, patients with HCV RNA < 25 IU/ml at W4 (undetectable or detectable) and < 15 IU/ml at W12 (undetectable) stopped treatment after W24 • Of the 225 (91%) patients who met RGT, 86% had SVR12 • Of the 16 who did not, 31% had SVR12 Manns M. Lancet 2014;384:414-26 QUEST-2
QUEST-2 Study: SMV + PEG-IFN + RBV for genotype 1 SVR12 (HCV RNA < 25 IU/ml) SMV Placebo p = 0.0031 all p < 0.0001 % 96 100 85 81 80 75 67 65 58 53 51 50 41 40 19 25 CC CT TT F0-F2 F4 F3 IL28B genotype Metavir fibrosis score N 75 42 142 71 40 21 195 102 36 17 17 15 • SVR12 by baseline HCV RNA • ≤ 800,000 IU/ml : 454/58 (93%) in SMV vs 81% in placebo ; p < 0.0001 • > 800,000 IU/ml : 155/199 (78%) in SMV vs 39% in placebo ; p < 0.0001 0 Manns M. Lancet 2014;384:414-26 QUEST-2
QUEST-2 Study: SMV + PEG-IFN + RBV for genotype 1 Virologic failure • Emergence of resistance among SMV-treated patients who failed to achieve SVR12 • Emergence of NS3 mutations in 41/42 (52%) • Genotype 1a (N = 16) : most common = R155K alone (N =13) or in combination (N = 2), or D168V (N = 1) ; 5/16 with Q80K at baseline • Genotype 1b (N = 25) : most common = D168V ; Q80R + D168E ; no Q80K at baseline • No impact of RBV dose reduction (24% of SMV and 31% of placebo) on outcome Manns M. Lancet 2014;384:414-26 QUEST-2
QUEST-2 Study: SMV + PEG-IFN + RBV for genotype 1 Adverse events Manns M. Lancet 2014;384:414-26 QUEST-2
QUEST-2 Study: SMV + PEG-IFN + RBV for genotype 1 • Summary • A significantly higher percentage of treatment-naive patients with chronic HCV genotype 1 infection achieved SVR12 (primary efficacy endpoint) with SMV in combination with PEG-IFN + RBV than with placebo in combination with PEG-IFN + RBV and has lower on-treatment failure and relapse rates • This superiority of SMV was seen irrespective of the type of PEG-IFN-alfa used • 91% of patients in the SMV group met criteria for response-guided therapy and were eligible to shorten treatment and stop at W24, and 86% of these subsequently achieved SVR12 • IL28B non-CC genotype, cirrhosis, and high baseline HCV RNA were associated with lower SVR rates • in patients with HCV genotype 1a • SVR12 was similarly high in patients with or without the Q80K polymorphism at baseline • However, SVR12 was significantly lower in placebo group overall vs SMV group with Q80K polymorphism (p < 0.05) • Most patients treated with SMV who did not achieve SVR12 hademergent mutations at the time of failure • Adverse events in the SMV group were clinically manageable, and mostwere grade 1 or 2. Discontinuation for adverse event was rare in both groups Manns M. Lancet 2014;384:414-26 QUEST-2



















