Download
1 / 58
580 likes | 584 Views
Postmenopausal Hormone Therapy after Women's Health Initiative Study: Oncologic Aspects VVOG – 27.09.2008 Brugge. Professeur Ulysse GASPARD Dept of Obstetrics and Gynaecology University of Liège - BELGIUM. Am I the right Walloon in the right place ?. I'll TRY and DO my best !.

E N D
Postmenopausal Hormone Therapy after Women's Health Initiative Study: Oncologic Aspects VVOG – 27.09.2008 Brugge Professeur Ulysse GASPARD Dept of Obstetrics and Gynaecology University of Liège - BELGIUM
Am I the right Walloon in the right place ? I'll TRY and DO my best !....
< 19.5 < 25.9 < 34.2 < 52.2 < 101.1 BreastAge-standardized incidence rate per 100,000 Globocan 2002, IARC
Globally, breast cancer is the most prevalent cancer in women ASR (incidence): 37.7 ASR (deaths): 13.2 New cancer cases (all ages), females 5,060,657 1151289 (22.7%) 493243 (9.7%) 472687 (9.3%) 386891 (7.6%) 330518 (6.5%) 204499 (4.0%) 198783 (3.9%) 184043 (3.6%) 146723 (2.9%) 1491972 (29.5%) http://www-dep.iarc.fr/ Globocan 2002, IARC
Oxford meta-analysis Randomized controlled trials Hormone therapyand breast cancer risk • HERS • WHI estrogen–progestin • WHI estrogen-only
Oxford meta-analysis (1997): 50,000 cases and 100,000 controls 2 0 Increased risk in current users Combined HT RR 1.53 (SE: 0.33) ≥ 5 years Estrogen HT RR 1.34 (SE: 0.09) No risk after 5 years since last use Relative risk (SE) < 1 1–4 5–9 10–14 > 14 Duration of use (years) CGHFBC. Lancet 1997; 350:1047
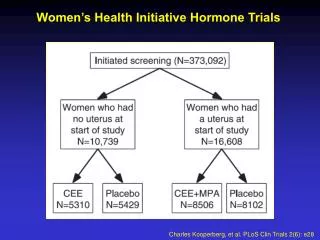
Randomized trials: description WHI WHICharacteristic HERS II E + P E n 1380/1383 8506/8102 5310/5429 Mean age (years) 67 63 64 Time since 19 15 > 10menopause (years) Previous HT 24% 26% 48%
Randomized, controlled trials: results HERS II WHI E + P E + P E Follow-up (years) 6.8 6.2 7.1 RR of BC (ITT) 1.27 1.260.80 95% CI 0.8–1.9 1.0–1.60.62–1.04 RR of BC (adherent) 1.490.67 95% CI 1.13–1.960.47–0.97 Hulley JAMA 1998; Chlebowski JAMA 2002, JAMA 2003; Stefanick, JAMA 2006
BC risk in WHI – I and -II • WHI-I = E-PRT (6.2 years FU)(1) • inv. BC 199 cases (E+P) vs 150 cases (placebo) • HR 1.24 (1.01-1.54) • 41 cases (E+P) vs 33 cases (placebo) p 10,000 WY • E-PRT : + 8 extra cases p 10,000 WY (0.08%) • E-PRT cases diagnosed at more advanced stage • WHI-II = ERT only (7.1 years FU)(2) • inv BC 104 cases (CEE) vs 133 cases (placebo) • HR 0.80 (0.62-1.04) P = 0.09 (NS) • 28 cases (CEE) vs 34 cases (placebo) p 10,000 WY • E-RT = - 6 cases p 10,000 WY (- 0,06%) • ERT treatment increased mammographic abnormalities (1) Chlebowski RT et al, JAMA 2003;289:3243 (2) Stefanick ML et al, JAMA 2006;295:1647
Discussion of the RRfrom ET and CEPT in the WHI • Differences in clinical characteristics, different population • Body mass index • Different percentage of drop-out in the two arms/trials: similar patients? • Differences in clinical characteristics between CEE and placebo groups: • Less bilateral oophorectomy: 39.5% vs. 42% • More first-degree relatives with breast cancer: 12.9% vs. 11.9% • Less biopsy for benign breast disease 19.3% vs. 21.7%
Body mass index: the risk with HRTis (more) apparent in lean women • Schairer et al., 2000:BMI > 24.4 kg/m2no additional risk • Rosenberg et al., 2006: BMI > 26 kg/m2 no additional risk • MWS, 2006: inverse relationship between the risk and BMI withERT and E-PRT • E3N cohort, 2005: 80% of users have a BMI < 25 kg/m2
HT and breast cancer risk: WHI effectsof previous treatment and duration 10 1 0.1 No previous treatment: no increase at 6 years 12,297 never users No prior use HR: 1.02 (0.77–1.36) 4311 prior users Prior use HR: 1.96 (1.17–3.27) Relative risk 1 2 3 4 5 6+ Duration (years) p = 0.02 Anderson GL et al, Maturitas 2006;55:103
Ravdin • Decrease began in mid-2002 and had begun to level off by mid-2003. • Decrease was evident only in women who were 50 years of age or older. • Mainly ER positive tumors Ravdin P et al, NEJM 2007;356:1670
Decrease not found everywhere Not in Canada, NL, UK?, Finland, Norway, Sweden… where screening is stable or low use of HRT?
Norway (Zahl & Maehlen, NEJM 2 August 2007) screening
Persistence of BC risk 3 years after stopping WHI E-PRT study After 3 years cessation : 42 cases (EPRT) vs 33 cases (plac.) = + 9 cases p 10,000 WY HR 1.27 (0.91 – 1.78) Heiss GSM et al, JAMA 2008;299:1036
Comments A non-event? Not so surprising that a promoter effect does not stop the day of the end of the treatment! Suggests that the effect is slowing progressively but 2.4-3 years is a too short period for recording any significant decrease incidence Does not fit the extremely rapid decrease in breast cancer incidence reported by Ravdin et others! Possible flaw: the number of women lost for the follow up?
Intermediate conclusions (1) • Weakly increased risk of breast cancer with E-PRT after 6 years of use, decreasing later on after cessation • No increase with ERT in RCT • But the risk factors were different between the E and E + P WHI trials • Role of estrogens in breast cancer is demonstrated: • from Beatson (1887) to the STAR study • Raloxifene decreases the RR of ER+ breast cancers by an antiestrogen effect
Intermediate conclusions (2) Longer time of exposure to ERT before BC risk is increased HRT acts as a promoter However risk factors may vary among women treated by EPRT or ERT (age, BMI, etc...etc...)
Differences in BC risk in PMW with different types of HRT • E alone • E oral or transdermal ? • E + Progesterone or synthetic Progestins • Tibolone
Estrogen alone (ERT)vs combined estrogen + progestin (E-PRT)
Type of study, country ERT E-PRT Meta-analysis Oxford 1996 Meta-analysis, UK 1.34 (SE 0.09) 1.5 (SE 0.33) Magnusson 1999 Case–control, Sweden 1.9 (1.5–2.6) 1.6 (1.4–1.9) Persson 1999 Cohort, Sweden 1.1 (0.6–1.6) 1.9 (1.3–2.8) Schairer 2000 Cohort, USA 1.1 (1.0–1.3) 1.3 (1.0–1.6) Ross 2000 Case–control, USA 11 (1.0–1.2) 1.2 (1.1–1.5) Porch 2002 Cohort, USA 1.0 (0.7–1.4) 1.4 (1.1–1.8) Chen 2002 Case–control nested, USA 1.2 (0.9–1.6) 1.5 (1.0–2.1) Weiss 2002 Case–control, USA 0.8 (0.7–1.1) 1.2 (0.9–1.5) Olsson 2003 Cohort, Sweden 0.7 (0.4–1.3) 1.2 (0.7–2.0) Li 2003 Case–control, USA 1.0 (0.8–1.3) 1.7 (1.3–2.2) Million Study 2003 Cohort, UK 1.3 (1.2–1.4) 2.0 (1.9–2.1) Bakken 2004 Cohort, Norway 1.8 (1.1–2.9) 2.5 (1.9–3.2) Stahlberg 2004 Cohort, Denmark 1.96 (1.16–3.35) 2.70 (1.96–3.73) Fournier 2005 Cohort, France 1.10 (0.8–1.6)* 1.3 (1.1–1.5) *increased by ≥ 6 years Ewertz 2005 Cohort, Denmark 1.35 (1.01–1.80)1.05 (0.62–1.79) Chen 2006 Cohort USA (ER+) 1.48 (1.05–2.07)* * ≥ 15 years MWS 2006 Cohort, UK 1.3 (1.2–1.4) 2.14 (2.04–2.24) Dinger 2006 Case–control, Germany 0.8 (0.7–1.0) 1.2 (1.0–1.3) Lyytinen 2006 Cohort, Finland 0.93 (0.80–1.04) < 5 years1.44 (1.29–1.59) ≥ 5 years
Million Women StudyERT vs E-PRT and BC • 1,084,110 UK women, 50–64 years old • Recruited from mammography screening • Initial questionnaire on treatment, re-evaluation after 2.8 years only in a subset of 12,221 patients • Ever users: RR: 1.43 (1.36–1.50) • Current users: RR: 1.66 (1.58–1.75) • Past-users: RR: 1.01 (0.94–1.09) • ERT users: RR: 1.30 (1.21–1.40) • E-PRT users: RR: 2.00 (1.88–2.12) Beral V. et al, Lancet 2003;362:419
E-only therapy and risk of BC Nurses'Health Study (cohort) Prospective cohort study 19802002 n = 28835 PMW with hysterectomy (E alone or no HRT) n = 934 inv. BC • RR ERT vs no use : < 5 years 0.96 (0.75 – 1.22) NS 5-9.9 years 0.90 (0.73 – 1.12) NS 10-14.9 years 1.06 (0.87 – 1.30) NS 15-19.9 years 1.18 (0.45 – 1.48) NS > 20 years 1.42 (1.13 – 1.77) Signif • P trend for current use over time : P < 0.001 Increased risk of BC with ERT ONLY after LONG TERM use (15-20 years) Chen WY et al, Arch Intern Med 2006;166:1027
Oral vs transdermal estrogens and BCUK GP database Population case-control study, 1988-2004 Women 50-75y ( 22% hysterectomy) 6347 BC (age:61y) and 31,516 controls Opposed E2 oral form RR 1.38 (1.27–1.49) patch form RR 1.08 (0.81–1.43) Estrogens+ progestins: RR:1.38 (1.27–1.49) Pregnanes RR 1.53 (1.22–1.92) Norsteroids RR 1.29 (1.18–1.40) Opatrny L. et al, BJOG 2008; 115:169
Oral estradiol vs transdermal Finnish study From cancer registry 2,171 cases of breast cancer SIR 0.93 (0.80 –1.04), < 5 years SIR 1.44 (1.29 –1.59) > 5 years (1) Oral and transdermal estradiol similar increase in the riskafter 5 years increase with dose > 1.9 mg/d orally risk associated with transdermal route not dose-dependent. (1) SIR = Standardized incidence ratio Lyytinen H et al, Obstet Gynecol 2006;108:1354
Different types of Progestins and risk of BC in PMW Northern Europe • Predominant E2 + NETA (78% Norway) USA • Predominant CEE + MPA France • Predominant E2 + natural progesterone (25%)
Specificities of progestogens Natural Agonist Antiestrogenic activity Antiandrogenic activity Progesterone CPA DRSP progesterone Progestogens Estrogenic activity NETA LNG Androgenic activity LNG NETA MPA MPA MGA Pregnanes CMA = Chlormadinone acetate MGA = Megestrol acetate CPA = Cyproterone acetate MPA = Medroxyprogesterone acetate Norsteroids NETA = Norethisterone LNG = Levonorgestrel DRSP = Drospirenone Glucocorticoid activity Progesterone DRSP Antialdosteronic activity
Million Women Study in the UK No difference between • Norsteroids (norgestrel/norethisterone acetate) • Pregnane (MPA) • Dydrogesterone • E2 oral or transdermal
Different types of Progestins and BC risk in PMWE3N -Population studied N women 80 391 N Person-years 653 125 Mean duration of FU 8.1 years (sd 3.9) N BC cases 2355 Histological confirmation 96.2% Hormone Receptor status 79% Fournier A et al, Breast Cancer Res Treat 2008;107:103
E3N – Types of HRT used in 2002 in France Courtesy of F.Clavel
E3N: Results • Estradiol and progesterone • RR = 1.00 (0.83–1.22), n = 129 • No increase with E2 + dydrogesterone • RR = 1.16 (0.94–1.43), n = 108 • Estradiol and synthetic progestin • RR = 1.69 (1.50–1.91), n = 527 • Estrogens alone whether ORAL or TRANSDERMAL • RR = 1.29 (1.02–1.65), n = 76 • 80% of users have a body mass index < 25 Fournier A et al, Breast Cancer Res Treat 2008;107:103
E2 + Progesterone does not increasethe risk at 8 years • Is it related to the regimen: transdermal E2 + P? • Is it related to a subset of patients? • Is it related to the specific clinical attitudeamong physicians who prescribe this regimen?
Pooled analysis: sequential vs continuous HRT 5/6 cohort studies E2+NETA C Cohorts S C Cases-controls 4/5 case-control studies CEE+MPA S 0.5 1 1.5 2 2.5 3 Global Analysis : NS G.Plu-Bureau & A. Gompel, IMS, Madrid, 2008
Tibolone and Risk of BC in PMW • UKGP Database(1) : • Tibolone only vs controls 0.86 (0.65 – 1.13) • Tibolone preceded by estrogen only 1.22 (0.74 – 2.00) • Tibolone preceded by E-PRT 1.29 (1.09 – 1.52) • LIFT study(2) RCT n = 2267 Tibolone vs 2267 Placebo mean age 68 years; FU 34 months RH 0.32 (0.13 – 0.80) P = 0.02 • LIBERATE study(3) RCT of BC survivors n = 1579 Tib vs 1569 Plac mean age 53 years FU 3 yrs RH 1.40 (1.14 – 1.70) P = 0.001 (1) Opatrny L et al, BJOG 2008;115:169 – (2) Cummings SR et al, NEJM 2008;359:697 – (3) Clinical Trial Report Liberate Study, Schering Plough Organon, May 2008
Different types of HRT and risk of BC Conclusions (1) • Suggestion of no increased risk with E2+Progesterone HRT (E3N) • Possible different mechanisms between Progesterone and synthetic progestins • Complexity of progestin actions linked with their non selectivity and individual responses
Different types of HRT and risk of BCConclusions (2) • No study can conclude with a level 1 degree of evidence about the relative risk associated with the use of different progestins • Different estrogens carry a comparable moderate dose-dependent increased risk
Histopathological typeof breast cancer during HRT Lobular carcinoma
HRT and Ductal vs Lobular BC (Li & Daling Cancer Epidemiol/Biomarkers Prev 2008)
E3N and BC Type RR for HRT ever use vs. never use Ductal Lobular E E+P4 E+Dy E+P∑ E E+P4 E+Dy E+P∑ P homogeneity <0.001<0.02 Courtesy of F.Clavel Fournier A et al, J Clin Oncol 2008;26:1260
The so-called "promoting effect of HRT" could also be related to An increase in breast densitydelaying the diagnosis
Risk factors, RR 2–4 High risk Low risk Mother or sister Yes No Benign breast disease Yes Nowithout atypia Breast density > 75% Yes No Thoracic radiotherapy Yes No
Density • Spontaneouslyincreased density: RR increased 3–6 times • Density during HRT (÷ to E dose and E+P) • Edema • Stroma (androgens?) • No increase in proliferation • Breasts with increased density Leads to increased frequency of mammograms Mc Tiernan A. 2005; Kerlikowske K. 2005; Barlow W. 2006; Johansson H. 2007; Von Schoultz B. 20007
E-PRT > ERT better differentiated tumors bias of screening "only 10% of hormone therapy users had never been screened compared with 30% of never hormone therapy users" Better PROGNOSIS of cancer under combined E-PRT and ERT
Fatality rateafter 5 years of HRT vs. no HRT (2,347 deaths/12,836 breast cancers) Treatment Hazard ratio E, cyclic, combined HT 0.4 Long cyclic HT 0.3 Continuous combined HT 0.7 Tibolone 0.5 All 0.5 Lidegaard, DaHoRS (Danish Sex Hormone Register Study), Istanbul, EMAS 2006
Mortality from breast cancer and treatments Any HT former 0.86 (0.73-1.01) HT current RR: 0.74 (0.65-0.85) EPT current RR:0.59 (0.47-0.75) ET current RR:0.81 (0.68-0.96) (Newcomb et al CEBP 2008)
PROGNOSIS of breast cancerin HRT-treated women • Most studies, except the WHI study, show a better prognosis of breast cancer in HRT-treated women (size, n, grade), and an improved survival
Risk of colorectal cancer and hormone use in the WHI Studies I and II E – PRT : • n = 8506 E-PRT users vs 8102 placebo; mean FU 5.6 yrs • n = 43 colorectal Ca in hormone users vs 72 in placebo group • HR = 0.56 (0.36-0.81) p = 0.001; similar after adjustment for 7 outcomes • 9 cases p 10,000 WY (E-PRT users) vs 16 cases p 10,000 WY (placebo) = - 7 cases p 10,000 W per year due to E-PRT protection(1) ERT : • n = 5310 ERT users vs 5429 placebo; mean FU 6.8 years • n = 61 (ERT) vs 58 (placebo) colorectal cancer • HR = 1.08 (0.75-1.55) NS; similar after adjustment • 17 cases (ERT) vs 16 cases p 10,000 WY • No protection with ERT use(2) (1) Chlebowski RT et al, NEJM 2004;350:991 – (2) WHI steering Comm, JAMA 2004;291:1701
Colorectal Cancer and EPRT in WHI Chlebowski RT et al, NEJM 2004;350:911