Download
1 / 33
330 likes | 338 Views
Research on HIV risk among gay, bisexual, and other men who have sex with men. Barry D Adam University Professor Senior Scientist & Director of Prevention Research. Conceptualizing HIV risk. Epidemiology Postulating MSM category Identifying general trends Risk factor analysis:

E N D
Research on HIV risk among gay, bisexual, and other men who have sex with men Barry D Adam University Professor Senior Scientist & Director of Prevention Research
Conceptualizing HIV risk • Epidemiology • Postulating MSM category • Identifying general trends • Risk factor analysis: • Search for pathological causal factors, often abstracted from context • Rational man compromised by intervening variables • Biomedical or psychological individualism
The “calculating, rational, self-interested subject” (Smart 2003:7), the paradigmatic subject of contemporary neoliberalism • contract-making citizen • choice-making consumer (Habermas, 1987) • in health research, • the rational, conscious, informed calculator of risk
Health research models • Theory of reasoned action, health belief model • Subjects, “portrayed as free actors who are constrained only by their ignorance about the threat to which they may be exposed or their lack of self-efficacy” (Lupton, 1999, p. 23) • Or as an “audience of thoughtful, actuarial subjects, gathering data and acting on the basis of ‘fact’” (Davis, 2002, p. 281)
Socio-cultural analysis • How to cope with an unwanted health threat while searching for human connection • How to find pleasure and love while navigating sometimes conflicting sources of risk and opportunity • Cultural resources/discourses available to make sense of risk, choice & health • How social environment (state, capital, social institutions) shape cultural resources
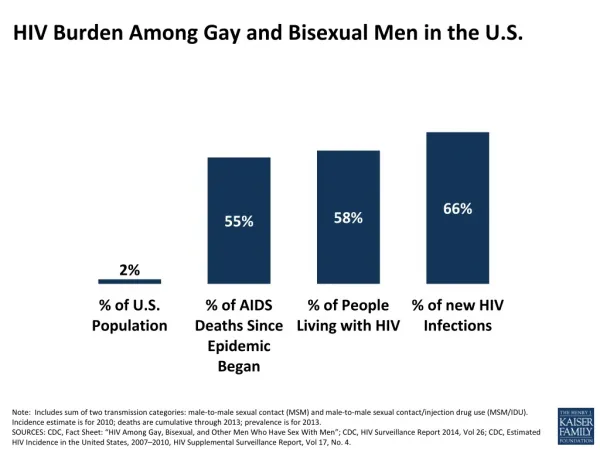
What Are The Numbers? • At the end of 2006, MSM accounted for 76.1% of cumulative reported AIDS cases among adult males. • Since 1985, MSM accounted for 68.8% of positive HIV test reports among adult males. • In 2005, MSM accounted for an estimated 45% of all new infections in Canada. http://www.phac-aspc.gc.ca/aids-sida/populations-eng.php#men
Public Health Agency of Canada. HIV/AIDS Epi Updates, November 2007, Surveillance and Risk Assessment Division, Centre for Infectious Disease Prevention and Control, Public Health Agency of Canada, 2007. • An estimated 2,300 to 4,500 new HIV infections occurred in 2005, and MSM accounted for the greatest number of these new infections, 1,100 to 2,000 • 27% of the estimated number of Canadians living with HIV infection at the end of 2005 are unaware they are HIV+ http://www.phac-aspc.gc.ca/aids-sida/publication/epi/pdf/epi2007_e.pdf
Ontario • HIV prevalence: 16% (but varies by region: 6 -21%) • Translates to >800 new HIV infections annually • Robert S. Remis and Juan Liu. 2007. Epidemiologic trends in HIV infection among men who have sex with men in Ontario. http://www.phs.utoronto.ca/ohemu/doc/MSM_Sept_2007.pdf • Highest infection rates among men, 20-50
Risk context age, identity, social class physiology ethno-cultural socio-cultural psychology sexual communication settings circuits drug use
Psychological factors • Sex abuse • Sensation seeking • Personal disruption, stress & depression • Social isolation
Sex abuse • Men reporting unprotected anal intercourse (UAI) more likely to report childhood sexual abuse • HIV+ men report more childhood abuse than HIV- men • Domestic abuse more common among men with UAI • Also a predictor of drug use, more sex partners, sex work
Sex abuse • Social context: “Young Latino boys who are gay or effeminate may be at greater risk for CSA than those who are not.” (Arreola & Díaz 2002) • Difficulty asserting condom use with an abusive partner • “Depression, confusion and uneasiness about sex, and even loss of control over their love lives, make meaningful self-protection more difficult.” (Dorais 2004:119)
Sensation seeking • = e.g. bungee jumping, skiing fast, known as a risk taker, fast driving, easily bored • Personality trait and/or expression of sexual exploration & youthful party-hard experience?
Personal disruption, stress & depression • Low-grade depression & UAI • Major stressors, i.e. job loss, moving, death of partner, etc • When life is worth living • Planning for a healthy future
Social isolation • Lack of social support, loneliness & UAI • Fatalism & UAI • "To the extent that persons do not hold positive views for their future, and to the extent that life is currently lacking satisfaction, motivation to initiate and maintain risk reduction changes in likely to be weaker." (Kalichman et al. 1997:545)
Drug use • UAI & “club drugs” • Alcohol with or without drugs • Poppers • Drug use & condom breakage • Drug use & recent seroconversion
Drug use causal? • Does drug use cause UAI, therefore we should campaign against it, or is drug use a way of dealing with several problems? • Drug use + “sexual escape expectancies” • "in only three cases was this [drug use] stated in isolation, the rest feel that emotional issues had resulted in the use of drugs/alcohol as a means of release/escapism" (Gilbart et al. 2000)
“Risky sex does not result from the simple exposure to drugs or alcohol before or during sexual behaviours, but rather depends on mitigating factors such as the personal convictions of the individual, as well as the decision-making processes that occur well throughout the sexual act.” (Myers et al. 2004:225)
Crystal meth • “three main patterns to respondents’ motivations to use crystal: escaping loneliness, dealing with feelings of sexual unattractiveness, and lowering sexual inhibitions. In a more general sense, these problems appeared to stem from deep-seated feelings of being unloved and unlovable.” (Kurtz 2005:65)
Circuit parties & • “tribalism,” “esprit de corps,” and sense of communion associated with club drugs
Sexual communication • Couples • Trade offs • Disclosure
Becoming a couple • Condoms dropped over time as sign of trust • “Negotiated safety” vs tacit move
“Sero-discordant” couples • Not wanting to stigmatize a HIV+ partner • “In the context of relationships where one partner is HIV positive, unprotected sex can be considered to communicate feelings of ‘love’ and ‘commitment’ in even more powerful ways than would be the case if both partners were negative.” Rhodes 1997:215
Setting • “rules of engagement” in quick sex environments: • Low disclosure • Low sense of obligation to partners • i.e. market rules; buyer beware
Disclosure • Cuerrier & disclosure • Greater with better-known partners; less with casual • Safer sex practised more often with casual partners anyway • Disclosure is not associated with higher rates of protected sex • Those who decide, encounter to encounter, whether to disclose or not, and who then disclose inconsistently have higher rates of UAI
Circuits & microcultures • Internet & more UAI but internet users no more likely to have UAI with partners met on-line than off • Barebacking and “rhetoric of individualism, personal responsibility, consenting adults, and contractual interaction.” (Adam 2005)
Bareback circuit “Participants tacitly signed onto the social contract that states the primary responsibility to disclose HIV status is placed on the sexual partner. Many claimed to operate from the assumption that people are responsible for their own bodies, and that feelings of responsibility toward another are not obligatory. The participants referred to an ‘unspoken rule’ that men in public sex environments who did not initiate a discussion on disclosure were either HIV-infected or did not care about their health.” Reback et al 2004:94
Condoms vs erections Condom-avoidance rationales: • desensitizing • symbolic value of insemination • Intimacy • Erectile difficulties more common in older men and men on HAART • Viagra & UAI
HIV optimism • Low endorsement among gay men • Cause or post hoc rationalization? • Rarely arises in narratives about UAI • Same as “undetectable” viral load? • Indicator of bareback circuit?
Socio-demographics • Youth • Bisexual men • Lower education & income • Migration & cultural assumptions • Men of colour & culturally appropriate communication
Trade offs • scenarios where men who feel disadvantaged in some way—be it age, ethnicity, or attractiveness—fear to offend a desirable partner and trade away safe sex lest it prove an obstacle to sexual interaction
What’s missing? • Insufficient study of institutional sources of HIV information • Schools, mass media, churches/mosques, biomedicine • Inadequate mapping of popular understanding of HIV technologies and messages • For example, claim that gay men are complacent because of ARVs–widely propagated, poorly documented • How does treatment=prevention mantra propounded by biomedical “experts” translate into everyday risk management?
Insufficient ethnography of most vulnerable subsets of at-risk populations. • Not “behaviour,” but practices embedded in exigencies and choices of everyday life • Not “inadequate uptake” or failure to be rational, but discourses available for making sense of risk • In short, it’s about social networks, and sexual and drug cultures