Download
1 / 47
470 likes | 701 Views
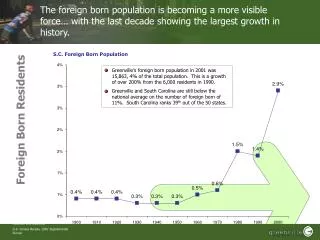
Foreign-born uninsured women and prenatal care. New Mexico Pregnancy Risk Assessment & Monitoring System Presenter: Ssu Weng Maternal & Child Health Epidemiology Conference December 2003. PRAMS Susan Nalder, Director NM PRAMS Dorin Sisneros, Operations Manager NM PRAMS

E N D
Foreign-born uninsured women and prenatal care New Mexico Pregnancy Risk Assessment & Monitoring System Presenter: Ssu Weng Maternal & Child Health Epidemiology Conference December 2003
PRAMS Susan Nalder, Director NM PRAMS Dorin Sisneros, Operations Manager NM PRAMS CDC PRAMS team – Nedra Whitehead NM PRAMS Steering Committee NM Office of Vital Records Kimberley Peters, Brian Woods; formerly with NMVR: Vicky Howell NM Department of Health Survey Unit Mothers who responded Funding sources and sponsors CDC Cooperative Agreement U50/CCU613632-03 Title V MCH Block Grant, NM Dept of Health Family Preservation and Support Project (NM Children Youth and Families Department) Joint Powers of Agreement with Medical Assistance Division (NM Department of Human Services) AcknowledgmentsOpinions in this presentation do not necessarily reflect official views of these individuals or organizations
Epidemiologic paradoxForeign-born women v. US-born • Demographic and socioeconomic risks • Outcomes Similar: low birth weight and infant mortality • Singh et al. 1996; Cervantes et al. 1999; • Guendelman et al. 1999; Fuentes-Afflick et al. 1998; Buekens et al. 1998 • Better birth outcomes than state-born: • preterm delivery, low birth weight, teen birth • Sappenfield et al., MMWR 51:1091-5(Dec. 6 2002) • MCHEP presentations • Maternal characteristics and behaviors • Allen et al., in progress • Adequacy of prenatal care Mitchell and Denk
Original purpose of study • Goal • Provide data for PNC network taskforce • Seek Medicaid coverage for undocumented pregnant women • Compare • “Undocumented” with • Women who had Medicaid for PNC • But legal and citizenship status unavailable • Foreign-born may not be immigrant • No information on documentation
Revised questions • Independent variable • Foreign-born uninsured • No attempt to identify undocumented • “Outcomes” - were there differences in • Maternal characteristics • Access to and utilization of PNC • Outcomes of mother or infant
Methods • Two sources of data • Birth certificates for • Demographics • Prenatal care entry and visits • Infant’s birth weight • PRAMS: maternal behaviors, healthcare, hospital stay • Both: maternal medical risks, gestational age • Descriptive study • Later, select outcome(s) for multivariate analysis • Survey analysis • Stata: svymean, svylc to test for statistical significance • Display of data • Charts show 95% confidence intervals • Data tables with p-values on request
What is PRAMS? Survey of new mothers, led by CDC, 32 states Ongoing since 1987 (NM since 7/97)
NM PRAMS frame • Population-based • From NM Vital Records live births • NM resident mothers ~27,000 in year 2001 • Exclusions • Out-of-state births • Multiple births >3 • Adoptions
Survey design • Stratified systematic sample • Approximately 1/12 of frame • Over-sampled from year 1997-2000 • Low birth weight infants • Native Americans • Equal allocation from year 2001+ • Stratified by geographic region • Weighting at CDC based on • Response rates • Sampling fraction • Non-coverage
Data collection • Mailed survey: three times • Telephone follow-up interviews • 70.0% overall response rate, weighted • 68.4% foreign-born (65.6% if Hispanic) • 70.6% US-born
Definition “Foreign-born uninsured” • Maternal country of birth • U.S. states, excluding territories • Foreign: ~75% from Mexico • Payer of prenatal care • Uninsured: 2 groups, foreign- or U.S.-born • No Indian Health Service (IHS), Medicaid, or private insurance • Insured – hierarchy of payers • IHSMedicaidprivate • Combined foreign- and U.S.-born
Five groups: US-born dividedFocus on comparing group #1 with #2 or #3 • Foreign-born uninsured • US-born, uninsured • Medicaid paid prenatal care, no other payer (“Medicaid”) • Indian Health Service (“IHS”) • Private insurance, includes HMO, military
Sample and population Births July 1997-Dec. 2001 7310 respondents Restrict to 7150 mothers of singletons 232 missing data for country of birth or payer
Maternal characteristicsChallenges and advantages (?)US-born uninsured: standard errors > 2.5%
Maternal and family characteristicsand experiences • Intention of pregnancy • Smoking cigarettes, drinking alcohol • Partner abuse • Stressful experiences • Social support • Medical risks: diabetes, BMI, hypertension
Intended pregnancy% of mothers who wanted the pregnancy sooner or then
Unwanted pregnancy% of mothers who did not want the pregnancy then or ever
Alcohol% of mothers who drank frequently or binged during the 3 months before pregnancy
Cigarettes% of mothers who smoked during the last 3 months of pregnancy
Stressful events% of mothers with 6 to 12 stressful experiences during the 12 months before delivery
Stressful experiences% of mothers with each stressful experience by payer-birth country Standard error > 2.5% for several estimates for US-uninsured
Partner abuse% of mothers physically abused by partner during 12 months before pregnancy
Social support% with help raising the baby from husband/partner or family/friends
Maternal medical risks% of mothers who were hospitalized during pregnancy
Medical risks% overweight before pregnancyBMI>25.9kg/m2Signif. higher than US-born uninsured
Access to and utilization of care • Entry to PNC • Adequacy of PNC • Satisfaction with time of entry • Facility providing PNC • Medicaid as payer of labor & delivery
Late entry to prenatal care % of mothers starting after first 3 months of pregnancy
Cultural factors?Among women with late/no PNC, % who started as early as desired
Adequacy of prenatal care% with inadequate levelKotelchuck index % with intermediate level similar for all groups
Delivery – safety-net lackingAmong foreign-born without prenatal payer, % with delivery paid by these sourcesMultiple responses allowed and not all shown 58.5% 6.0% did not have third-party payer or indigent fund
Outcomes • Infant: birth weight, gestational age, nights in hospital • Mother: problems during pregnancy, hospitalization during pregnancy
Infant’s birth weight (BW)% of mothers with infant in each BW category by PNC payer/maternal birthplace Cells shaded to indicate significant difference between foreign-born uninsured and Medicaid. Other differences not significant.
Infant’s gestational age (GA)% of mothers with infant in each GA category by PNC payer/maternal birthplace Cells shaded to indicate significant difference between foreign-born uninsured and Medicaid. Other differences not significant.
Hospital stay • Mother • Median number days same for all groups • Mean difference n.s., although point estimate lower for foreign-born unininsured than Medicaid • Infant • Admission to ICU similar for all groups except private insurance, which was lower than foreign-born uninsured • Stay for 6 days or more: n.s. difference
Paradox: Foreign-born uninsured are challenged • Socioeconomic factors • Education • Income • Homelessness • Divorce, partner abuse before pregnancy • Access to and utilization of prenatal care • Financial barriers • Language • Late entry • Inadequate utilization
ParadoxOutcomes comparable or better compared with Medicaid mothers • Low birth weight < Medicaid • Preterm delivery < Medicaid • Newborn stay in ICU n.s. difference • Nights in hospital n.s. difference
Factors contributing to outcomes Foreign-born uninsured: • Behavior - less likely to • Smoke cigarettes • Use alcohol • Social issues • Stressful events • Attitudes: intended pregnancy • Healthcare resources • Community health centers
Implications for practice and policy • Community health centers and public health clinics play important role in prenatal care • Payer of delivery needed for 60% of foreign-born uninsured • Adequacy of prenatal care • Requires motivating women to get PNC
Paradox – not always? Future studiesRole of financial access to care • Foreign-born uninsured sometimes resemble US-born uninsured • Need to consider financial situation as well as country of birth
Paradox – exception?Future studies: HBW and LGA • Large for gestational age (LGA) • HBW data: increased risk among foreign-born uninsured? • Maternal BMI higher • Multivariate study • Binary • Compare with appropriate for gestational age (AGA) • Exclude SGA • Or multinomial model • Refine definition of AGA • Standards specific for maternal ethnicity/race and infant’s sex • Fetal or newborn measures?
FutureOutcomes based on data from sources outside PRAMS • Mortality • Birth defects: neural tube • Hospital discharge data • Length of stay • Diagnoses • Outcomes leading to cost estimates • Compare foreign-born uninsured with and without Medicaid-paid delivery
Limitations • Potential misclassification of payer • Within prenatal period, time period not specified for multiple payers • Medicaid outcomes • Uninsured US citizens with medical risks may shift to Medicaid during pregnancy • “Healthy immigrant” effect
Limitations • Lower rates of hospitalization • Role of provider’s practices • Response or non-response • Admitting or denying high-risk behaviors • Out of state births excluded • Higher risk? Foreign-born? • In 1998 • 3.6% of all resident births • 19% of Dona Ana resident births • Analysis by domains • Potential duplicates in combined years
NM PRAMS Contacts Susan Nalder • MCH Epidemiology Program Manager & • NM PRAMS Director • Tel 505 476 8889 • susann@doh.state.nm.us NM PRAMS Coordinator (S. Weng) • Tel 505 476 8895 • nmprams@doh.state.nm.us Ssu Weng, Epidemiologist • Tel 505 476 8892 • ssuw@doh.state.nm.us MCH Epidemiology Program Family Health Bureau NM Department of Health 2040 South Pacheco St. Santa Fe, NM 87505 www.state.nm.us/doh/prams/home.html