Download
1 / 25
270 likes | 462 Views
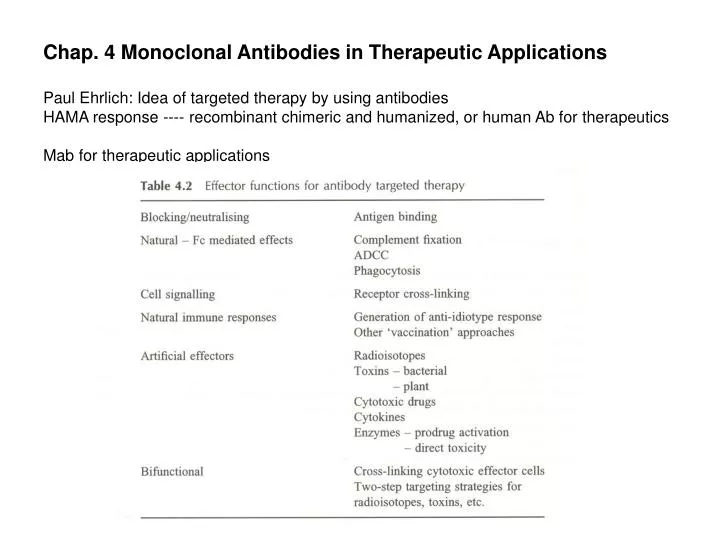
Chap. 4 Monoclonal Antibodies in Therapeutic Applications Paul Ehrlich: Idea of targeted therapy by using antibodies HAMA response ---- recombinant chimeric and humanized, or human Ab for therapeutics Mab for therapeutic applications. Cancer

E N D
Chap. 4 Monoclonal Antibodies in Therapeutic Applications Paul Ehrlich: Idea of targeted therapy by using antibodies HAMA response ---- recombinant chimeric and humanized, or human Ab for therapeutics Mab for therapeutic applications
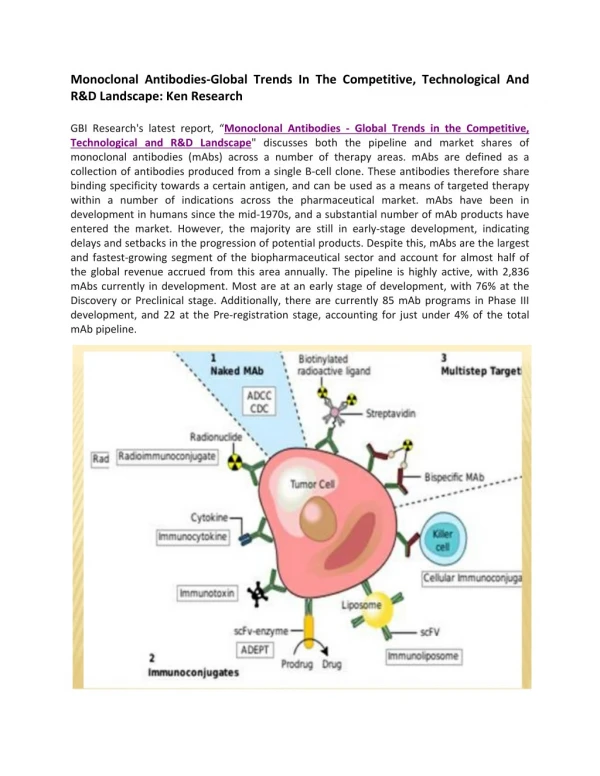
Cancer [1] Cancer therapy with unmodified (naked) antibodies Harness natural effector functions (tumor cell killing) a) selection of suitable isotype i. mouse IgG2a --- human ADCC ii. human IgG1 & IgG3 --- cell killing (IgG1: construction of humanized Ab) iii. CHO on CH2 --- important for eliciting the effector function Ab as ligands eliciting anti-tumor effects by signal transduction --- arresting cell cycle or inducing programmed cell death Ab to growth factor receptor or GF (EGF and IL-6) --- blocking GF-mediated tumor cell growth Dimeric or polymeric Ab via X-linking --- complement activation and ADCC enhancement (homodimer – signalling activity for cell cycle arrest or apoptosis) Not successful, but it’s promising. a) CAMPATH-1H (the first humanized CDR-grafted antibody) --- complement activation against B-cell lymphoma b) C2B8 against CD20 (B-cell surface phosphoprotein) --- complement activation, ADCC, cell signalling mech. (B-cell lymphoma) c) Ab against p185HER2 (transmemb GF receptor, HER2/neu/c-erb-B2) i. growth inhibition by down-regulating the GF receptor ii. signal transduction pathway leading to cell death iii. ADCC
[2] Anti-idiotype antibodies Vaccines to generate anti-idiotype response Anti-idiotype antibody carries “internal image” of original Ag [Ag – Ab1, Ab1– Ab2; Ab2(anti-idiotype antibody) – Ab3 (Ag recognition)] Vaccination with Ab2 for poorly immunogenic target antigens a) Ab induction via breaking immunological tolerance b) induction of T-cell response (therapeutic significance) i. 105AD7 (Ab2 mimicking a colorectal tumor-associated Ag) --- T-cell response on the turmor (delayed tumor growth and increased survival period) ii. murine Mab-17-1A (epithelial memb. Ag on colorectal tumor cells) --- anti-idiotype response in patients (high level of Ab3)
[3] Bispecific antibody-mediated effector cell targeting to recruit effector cells (Tc cells) to the tumor site Mechanism of targeting effector cells to tumors a) tumor recognizing antibody binding to Fc receptor on the effector cell b) bispecific antibody binding to markers on the effector and tumor cells
Activation of T-cell --- CD3/TcR complex in the presence of IL-2 & -7 plus co-stimulatory signals of CD2 and CD28 cf) trispecific antibody made by crosslinking three Fab’ fragments (tumor Ag and two different T cell antigens) Bispecific Ab via hybrid hybridomas, chemical crosslinking, recombinant DNA tech. (Bispecific diabody --- small size bringing the effector and tumor cells closer together) [4] Other approaches to recruit the immune system using monoclonal antibodies Superantigen (bacterial or viral proteins) --- [exotoxin from Staphylococcus aureus] a) most potent T-cell activator by recognizing both TcR and MHC-II on APC b) Fab’-superantigen fusion protein i. tumor cell targeting with T-cell stimulation (replacing MHC-II binding tumor cell binding) ii. T-cell infiltration and tumor attack increase iii. residual MHC-II binding property (problem causing high toxicity) mutations in the superantigen binding site for MHC-II Antibody-cytokine fusion protein (chimeric 14.18 --- tumor Ab-IL2 fusion protein) a) cytokine alone --- severe systemic toxicity b) fusion protein --- targeting a high local conc. of cytokine to the tumor site c) IL-2: T-cell proliferation and T-cell mediated killing TNFa, TNFb, GM-CSF, IL-5, IL-8, Interferon-a
[5] Radioimmunotherapy Tumor localization: 10% injected dose per Kg of tumor Toxicity (especially to bone marrow) To reduce the toxicity a) short-range radioisotopes (internalization for cytotoxicity) b) specific clearing mechanisms to remove circulating activity c) two-step targeting strategies d) use of rapidly clearing antibody fragments
Form of antibody • ideal molecule: (a) turmor localization in large amounts • (b) delivery of high dose of radiation • (c) rapid clearance from the circulation • (d) minimizing non-specific toxicity • F(ab’)2 or chemically cross-linked F(ab’)2 fragments [tumor penetration, phamacokinetics, • tumor accumulation] • cf) metallic isotopes --- intracellular accumulation or high levels in kidney • Chemically crosslinked tri-Fabs (TFM) • high accumulation in tumor, rapid clearance from the blood (Fc-), low level in kidney
(2) Radioisotopes (Table 4.5) isotopes with a high linear energy transfer (LET) [unlike the immunocytochemistry] a) Auger emitter – the highest dose of radiation, cellular internalization (short range) b) a-emitter – high radiation dose over a short range (50 mm in tissue) c) b-emitter – less energy, but long range (1cm – favorable for large tumor) d) g-emitter – no use for therapy, toxic to normal tissue (3) Clearance mechanisms and two-step targeting a) second Ab administration to remove hot Ab b) extracorporeal immunoaffinity chromatography column c) two step targeting protocols i. bispecific antibody for both tumor and DOTA-90Y Following removal of Ab, the isotope administration. ii. streptavidin labeled Ab for tumor – cleared via biotin-protein conjugate -- labeling with biotin-DOTA-90Y
[6] Immunotoxins (Ab-toxin conjugates) Protein toxins as potential cytotoxic agents for Ab targeted cancer therapy (protein synthesis inhibition via rRNA modification or EF-2 inactivation) Requirements of immunotoxins a) internalization b) small numbers of toxin molecules c) translocation (endosome or TGN) d) release of the toxin from Ab following internalization Subunits of toxin a) cell binding b) internalization c) toxic subunit
Conjugation via chemical linkage or expression of recombinant fusions (toxin gene to Ab gene) a) must be intact in the circulation, but be able to release free toxin inside the cell i. S-S bond ii. hindered S-S bond with methyl or phenyl groups iii. proteolytically sensitive peptide linker Optimal form of antibody a) intact IgG --- efficient internalization, high level accumulation at the tumor, but low tissue penetration b) Ab fragments (scFv, dsFv) --- more effective tissue penetration c) bispecific Ab --- tumor and toxin (saporin) [targeting, internalization, release] reduced nonspecific binding Clinical applications a) toxicity (hepatotoxicity, neurotoxicity, vascular leak syndrome) b) immunogenicity of protein toxins --- limits antitumor effects to remove the immunogenicity (immunosuppressive agents or PEGylation) use human enzyme as a toxin (human ribonuclease) --- no immune reponse poor cytotoxicity
[7] Drug conjugates Chemotherapy (cytostatic or cytotoxic drugs) little selectivity for tumor cells --- normal tissue toxicity (severe side effects) Target chemotherapeutic durgs via drug conjugates with antibodies less immunogenic compared to immunotoxins (small size) reduced non-specific toxicity (well-characterized drugs) Drug conjugation to Ab a) loss of activities of both Ab and drug b) poorly active immunoconjugates c) identify drugs of sufficient potency d) suitable chemistry to generate linkage between Ab and drugs without loss of activity (stable conjugates in circulation, release active drug during Ab degradation) e) many drug molecules per antibody f) polymeric carriers for drugs such as HAS or dextran before a site-specific attachment to antibody g) immunoliposome to target a large amount of the drug to the tumor PEG-modified phospholipid into the liposome --- reduced reticuloendothelial uptake (stealth immunoliposome) h) development of more toxic cytotoxic agent enediynes (calicheamicin), maytansinoids, tricothecenes, analogues of CC-1065
[8] Antibody-directed enzyme prodrug therapy (ADEPT) two step targeting method for cytotoxic drug therapy Disadvantages a) free drug may diffuse away from the tumor site --- affecting normal tissues b) no human enzymes or no extracellular enzymes to avoid activation of the prodrug in normal tissues (enzymes in Table 4.7) Carboxypeptidase G2 (CPG2) a) converting Glu derivative prodrug into nitrogen mustard drug b) three step system antibody-enzyme conjugate --- clearance with galactosylated Ab --- Prodrug (anti-CEA F(ab’)2-CPG2) c) use of small size conjugates such as scFv-enzyme fusions d) immunogenicity of the enzyme in humans i. humanized Ab ii. human enzyme iii. catalytic Ab (bispecific Ab with one for tumor Ag and the other with catalytic activity)
[9] Vascular targeting Shutting off tumor blood vessels --- tumor cell death by blocking effective blood supply a) anti-vascular approach --- targeting existing blood vessels and killing tumor endothelial cells i. Ab-toxin conjugate ii. blood clot formation by targeting tissue factor iii. markers of tumor vasculature --- endosialin and endoglin b) anti-angiogenic approach --- preventing the formation of the new blood vessels i. antibody for bFGF and VEGF and their receptors preventing tumor angiogenesis ii. antibody for the integrin avb3 (CD51/CD61) cell adhesion control (crucial for angiogenesis) apoptosis of the proliferating cells
Infectious disease [1] Antiviral antibodies a) RSV (respiratory syncytial virus) --- peumonia and bronchitis in infants neutralizing Mab against the surface Ab of F and G proteins of RSV i. long half-life of humanized IgG ii. Anti-RSV Ab from phage display (overcome the dominance of non-neutralizing epitope) b) HIV Fab against gp120 (the CD4 binding site) ---- CDR walking (CDR mutations to improve the affinity to pM range) Anti-HIV antibody i. prevention of the gp120/CD4 binding ii. Fc mediated phagocytosis of the virus iii. anti-gp120 immunotoxin (anti-gp120-ricin A-chain conjugate) [2] Bacterial Sepsis bacterial infection – endotoxin or LPS – inflammatory response – activation of host defense systems and release of inflammatory mediators (TNF and IL-1) – shock, organ failure, death a) Mab to endotoxin of all Gram – bacteria (lipid A component of endotoxin) murine IgM,E5 and human IgM HA-1A b) Mab to TNF --- inhibition of TNF (potential therapeutic for septic shock) Ab with human g4 (inactive isotype)
Blood Coagulation and Dissolution in dynamic equilibrium Blood coagulation following vascular injury --- Rapid and localized reaction (cascade) Hemostasis (the cessation of bleeding) a) vasoconstriction b) platelet aggregation c) fibrin clot formation d) fibrinolysis of the clot by plasmin [Overview] vascular injury platelet activation adhesion to the site of injury via von Willerbrand factor (collagen and gpIb/IX) platelet aggregation via fibrinogen (platelet gpIIb/IIIa) and plug formation fibrin clot formation through extrinsic pathway (negatively charged phospholipids) growth and maintenance of the fibrin formation by intrinsic pathway until the tissue repair
Cardiovascular disease [1] Inhibition of platelet aggregation Mab (mouse/human chimeric Fab fragment 7E3) against gpIIb/IIIa receptor on platelets blocking the interactions of fibrinogen and von Willerbrand factor --- no platelet aggregation Chimeric 7E3 Fab (ReoPro) prevents complications following angioplasty. 7E3 blocking --- reduced platelet crosslinking --- reduced platelet rich thrombus i. monovalent Fab, not bivalent IgG ii. chimeric Fab (CDR grafted humanized Fab) --- reduced immunogenicity iii. associated bleeding problem (heparin as anti-coagulant) [2] Thrombosis thrombolytic therapy with plasminogen activator (acute myocardial infarction) --- reocclusion and side-effects such as cerebral haemorrhage targeting thrombolytic agents to blood clots i. anti-Fibrin antibody and plasminogen activator (tPA or uPA) via chemical conjugation ii. fusion proteins such as scFv-uPA toward fibrin (not fibrinogen) iii. bispecific Ab (fibrin and tPA) to target PA to the clot iv. bispecific conjugate (bispecific di-Fab) anti-gpIIb/IIIa Fab’(7E3) and Fab’ recognizing tPA --- thrombolysis with anti-platelet effects
Disorders of the immune system and inflammatory diseases [1] The inflammatory response inflammation: the body’s protection reaction toward injury or the presence of foreign materials from infection inflammatory response via pro-inflammatory cytokines and cell adhesion molecules a) increased blood flow to the site b) dilation of blood vessels c) migration of lymphocytes across the vessel wall into the tissue Autoimmune disease (chronic inflammation) --- inappropriate T-cell activation towards self-Ag on APC Ab to T-cell or APC – potential therapeutics a) blocking T-cell activation b) cytokines (TNF) c) adhesion molecules (selectins and integrins) the long lasting IgG with neutral isotype blocking interactions in vasculature without the effector functions Parallel reagents: antibodies to the equivalent animal protein to generate information on potential efficacy
[2] Blocking inflammatory mediators a) Anti-TNF antibody Rheumatoid arthritis i. increased TNF level ii. endothelial activation and adhesion molecule expression iii. granulocyte activation (increased phagocytosis, degranulation, generation of oxygen radicals and prostaglandin E2) iv. stimulation of fibroblast growth v. stimulation of cytokine production vi. T-cell stimulation with IL-2 CA2 (mouse:human chimeric IgG1), CDP571 (engineered human IgG4) confirmation: reduction in pain, reduction in number of tender and swollen joints IBD i. Crohn’s disease ii. ulcerative colitis b) Anti-C5 (activated component of the complement system as mediator of inflammation) Ab blocking C5 i. no generation of the major chemotactic and pro-inflammatory factors C5a & C5b-9 ii. amelioration of inflammatory diseases (systemic lupus erythematosus) iii. anti-C5 scFv fragment : acute conditions (rapid penetration) myocardinal infarction/stroke/cardiopulmonary bypass
[3] Blocking adhesive interactions between vascular endothelium and leukocytes a) Ab to E-selectin on the endothelium without the Fc functions anti-inflammatory effects leukocyte interaction with E-selectin for the adhesion IgG4 (neutral isotype) Leu235Ala in the CH2 domain – reduced Fc receptor binding b) Ab to the leukocyte integrins and their receptors on the endothelium Ab to CD49d/CD29 (VLA-4) i. effects on multiple sclerosis (autoimmune disease with demyelination of CNS) ii. activated T-cells crossing the blood-brain barrier iii. block binding to CD106 (VCAM-1) and inhibit leukocyte migration [4] Antibodies which directly inhibit T-cell activation and proliferation a) T-cell receptor i. e–subunit of the CD3 complex: murine IgG2a (OKT3) potent immunosuppressive agent prevention of acute rejection ii. T-cell activation by OKT3 via crosslinking between CD3 of T-cell and Fc-receptor bearing cells iii. controlling immune response by OKT3 humanized OKT3 / IgG4 (human) / Leu235Glu in CH2 domain reduced T-cell activation and human therapy
b) CD4 (TcR and MHC II interaction) i. anti-CD4 antibodies : down regulation of T-cell activity and suppression of immune responses ii. non-depleting anti-CD4 antibodies : temporarily inhibit T-cell activation with major inhibition of other immune functions ex) primatized Ab (monkey-human chimeric Ab) c) IL-2 and its receptor interaction on Tc cell i. Ab for a-subunit (Tac receptor or CD25) ADCC activation prolongs the survival of heart transplants ii. Ab for b-subunit (IL-15 receptor) with Ab for a–subunit: synergistic effect leading to increased inhibition of T-cell proliferation iii. Bispecific Ab for both a and b subunits iv. Ab for g (IL-4 and –7 receptor subunit) d) Combining anti-CD3 and anti-IL-2 receptor a chain (CD25) i. bispecific Ab for CD3 and CD25 : effective immunosuppressant reduced toxicity by anti-CD3 Ab and inhibition of IL-2 interaction
e) Anti-CD25 antibodies i. therapeutics for graft versus host disease (GvHD) bone marrow transplantation mature T-cells from donor --- immune attack to the recipient’s tissues T-cell depletion of the marrow before the transplantation --- graft rejection 증가, relapse of leukemia, delayed reconstitution of the immune system anti-CD25(IL-2 receptor) Ab ---- loss of the IL-2 receptor on memory T-cells f) CD5 (all T cells and a subset of B cells) i. anti-CD5 Ab : depleting T cells (RA and GvHD therapy) ii. anti-CD5 immunotoxins (ricin-A) : T-cell internalization and cell depletion in vivo g) GvHD i. anti-CD25 antibody ii. anti-CD5 antibody iii. anti-CD3 F(ab’)2-ricin A chain conjugate : effective T-cell depletion iv. recombinant immunotoxin : anti-CD3 scFv – truncated diptheria toxin
[5] Antibody treatment of allergy allergic reaction : excessive immune response to a common normally harmless substance atopic individual sensitization by 1st allergen exposure --- 2nd exposure --- hypersensitivity reaction (high levels of circulating allergen specific IgE) Allergen --- IgE production from B-cell --- high affinity receptor binding on mast cells in tissue and bosophils in the circulation --- second exposure --- allergen crosslinks IgE molecules --- signal transduction and degranulation --- inflammatory mediators such as histamine, cytokines
a) Mab to IgE i. IgE at Fce receptor binding site ii. block binding to basophils and mast cells iii. down regulates Fce receptor on basophils b) Ab for specific allergens i. allergen on mucosal surfaces (nasal linings or lower airways) ii. neutralization of IL-5 inhibiting eosinophil infiltration in the lung ---- prevent tissue damage and hyperreactivity c) Ab to adhesion molecules (eosinophil migration into the lung) i. Ab to CD49d/CD29(VLA-4) inhibiting eosinophil accumulation and asthmatic response