Download
1 / 72
720 likes | 807 Views
Long Term Care Updates and Documentation Strategies. Tina Young, MSOT, OTR/L Older Adult MSG May 2010. Objectives. Introduction to the upcoming changes: RAC, MDS 3.0 and RUGS IV How they will affect OT practice?

E N D
Long Term Care Updates and Documentation Strategies Tina Young, MSOT, OTR/L Older Adult MSG May 2010
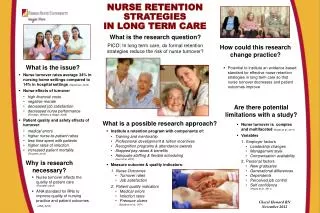
Objectives • Introduction to the upcoming changes: RAC, MDS 3.0 and RUGS IV How they will affect OT practice? • Documentation strategies with emphasis on the therapist rather than the client: Medical necessity, skilled services, measurable progress/goals, coding and more
Goals • Therapists will be able to state 2 upcoming changes in October 2010 • Therapists will be able to document better utilizing at least 5 strategies to prevent/minimize Medicare denials and improve our clinical practices • Therapists will understand the impact of our documentation on coverage and denials, protection of our skilled profession • Therapists will realize documentation is about the therapists’ skills, not just the client’s progress
Long Term Care Changes • RAC Recovery Audit Contractors Contracted through CMS Post payment review, identify improper overpayments after Oct 1, 2007 All providers are eligible to be audited, bills to Medicare Part A and B Collected over $1Billion in 3 years
Long Term Care Changes • RAC continued Demand letters are sent to Medical Records, if you don’t respond, expect 100% denial of claim They will apply the knowledge of Medicare rules and regulations to validate denials after reviewing the documentation They will take $ back!!!!
Long Term Care Changes • RAC continued Documentation can only use approved JCAHO abbreviations 2014 all documentation must be electronic nationwide Claims could be for illegibility or incorrectly spelled words
Long Term Care Changes • RAC continued Recommendations to consider: Each goal should have own attainment date Avoid “as per plan of care” and “patient tolerating tx well” Emphasize OTR/OTA collaboration, OTA should not document changes in plan of care or emphasis on…. without “collaboration with OTR”
Long Term Care Changes • RAC continued Transfer services from PRN therapists on evals Errors procedure must include: single line through item, word “error”, initials and date on each entry
Long Term Care Changes • RAC continued “OT evaluations can be denied if the following are not routinely noted on evals: Physiological status, cognitive baseline with a specific tool(s), communication status, specific testing of biom. measures. But due to the abbrev. ruling, such standard reporting as MMT cannot be reported in the abbrev., must be "manual muscle testing is 4/5 "(and then each assessment be interpreted), "indicating good muscle strength in order to support use of bilat UE in push off from toilet, bed" J. Winland’s AOTA CEU
Long Term Care Changes • MDS 3.0 CMS will adjust computations of ADLs, Eliminate section T of MDS (projections), OMRAs will be 1-3 days after therapy discharge (vs. 8-10 days) Beginning after October 2010
Long Term Care Changes • RUGS IV Beginning October 2010 66 RUGS (vs. 53)- new categories Modify the hospital “look-back” Update case-mix weights, nursing and therapy Change in coding therapy minutes on the MDS i.e. concurrent/group/individual
Long Term Care Changes • RUGS IV continued Nursing will have more brief interview section for cognition (MMSE) SLP will document signs/symptoms of swallowing deficits
Long Term Care Changes • Extension of Cap most likely beyond 12/31/10 deadline • Section 6121 mandates dementia care and abuse training for all SNF employees by 3/2011 • Incentives for prevention and wellness • Monitor readmissions to hospitals 1/2013 • CLASS Program developed rollout 2012
Long Term Care Changes • What do these 3 changes mean? Increase in Audits And Denials
Medicare Denials/Audit Process • Appeal process: Shortened time frame to appeal generally Within 120 days of receiving the initial determination denial to pay the claim found on MSN (Medicare Summary Notice), send a request for redetermination with all the documentation requested in the MSN and additional documentation that supports skilled therapy services such as: eval, treatment record, progress notes, discharge summary, orders nursing notes and physician signed POC
Medicare Denials/Audit Process Then you can appeal again with a reconsideration request, which is reviewed by a qualified independent contractor other than your Medicare payer, send documents and letter The third level of appeal is conducted by an administrative law judge, minimum of $110 in controversy The fourth level of appeal is the Medicare appeals Council, only if there was an error in the law or the case is a question of policy or procedure, minimum of $1090 controversy
Medicare Denials/Audit Process • Recommendations: Respond timely to denials Respond to ALL Medicare denials Prepare documentation/clinician to reduce denials as best defense (hone our documentation skills) All clinicians should be educated and understand the proper coding and essential documentation policies
Medicare Denials/Audit Process • Do NOT assume that the medical reviewer understands the level of sophistication of our skilled services. • Use materials to support the services that you are providing are within your profession, standards, guidelines, specialized knowledge and skills papers and evidences-based practice resources
Medicare Denials/Audit Process To Ensure Payment • Paint a Picture of the Patient with content not fluff • Be specific, clear and concise • Don’t write defer/refer to….. • Don’t leave blanks • Ask a therapist “can I read the note and know what to do next?”
Medicare Denials/Audit Process To Ensure Payment • Don’t write NT- you didn’t test for a reason, why • Use percentages, number of episodes • Document severity and impact of loss on whole person • Support reason for intensity (minutes of service)
Medicare Denials/Audit Process • Statements to avoid: Tolerated treatment well (assumption unless stated otherwise) Continue per plan of care As above Good/well Cognition interferes with therapy
Medicare Denials/Audit Process • Cognitive Aspects: Document skills of a therapist with education given, visual cues, establish compensatory strategies for safe return to…, able to recall…..spaced retrieval cues, use adaptations/compensatory strategies, strategies to reduce behaviors, address deficits that lead to functional loss, caregiver feedback, address the patient’s need for the goal
Medicare Denials/Audit Process • Addressing group therapy documentation Reason why for group, write clinical benefits, group addressed…… to improve…….
Medicare Denials/Audit Process • My recent experience with ADRs: Dementia diagnoses are most common Lack of cognitive scores UI treatment Lack of sufficient prior level status on evals Continuing goals met, lack of progress for a reviewer (in the FIMS section of notes) Group code, GO283 code, abbreviations, lack of supportive documentation from physician and nursing, where did referral come from
Relevant Transmittals that affect Documentation and denials Transmittal #63-documentation needs to be measurable and asks for functional assessment scores Recommend standardized test scores on evaluations and progress notes Show baseline and improvement correlated with function (what does the score mean?)
Relevant Transmittals that affect Documentation and denials • Transmittal #262 3 requirements for Medicare Coverage eligibility, MUST be met: Ordered service by a physician A skilled service is provided on a daily basis Service is reasonable and necessary
Relevant Transmittals that affect Documentation and denials • Transmittal #262 continued Dementia clients can make progress Allowed us to treat clients to their highest level
Relevant Transmittals that affect Documentation and denials • Transmittal #262 continued Stress remaining abilities that can be capitalized versus barriers d/t cognition Cognitive recall is not necessary to participate in this plan of care nor necessary for skilled intervention
Medical necessity Skilled services Referral from who, supportive documentation Physician order and certification Expectation of Improvement Standardized tests and correlation to function Goals-reasonable, predictable period of time Medical complexities Prior level Supervision/co- signatures Measurable Coding: ICD-9 and CPT Documentation: Focus is YOU
Documentation: Focus is YOU Need to answer in your documentation: Why should YOU be involved? What did YOU do? Did YOU analyze and adjust POC? Did YOU say that? Why are you needed (skills) vs. CNA”? HCR CEU
Documentation: Focus is YOU • Initial Evaluation: Document functional performance prior level and current level, standardized tests and relation to function (interpretation or analysis), all applicable medical diagnoses, ICD-9 codes, precautions, contraindications, specific problem areas being evaluated- body part,
Documentation: Focus is YOU • Initial Evaluation: Qualifications of a therapist needed to provide intervention, pertinent medical or therapy history to determine degree of functional loss, reason for referral-why evaluating
Documentation: Focus is YOU • Reasons for referral: Identify DME needed, identify number of medications, how mental/cognitive disorders impact the rate of recovery, cause of condition, symptoms, other health services concurrently being provided (dietitian, social services, nursing, hospital or physician consultations
Documentation: Focus is YOU • If you don’t document the reason for the referral, it can be denied as not medically necessary, we should discuss referral sources’ comments in our documentation to support our claim
Documentation: Focus is YOU • Evaluations are extremely important since 2/3 of denials are based on medical and skilled necessity • Document how to link medical diagnoses to functional changes, why have therapy?, medical dx alone doesn’t say what we are doing for the patient • Age, severity, time of onset • Expectation of improvement
Documentation: Focus is YOU • Add social, psychological and medical stability, motivation, acuity of condition, prognosis, complexity of condition, explain why progress may be slower secondary to medical conditions and co morbidities, patient self report
Documentation: Focus is YOU • Medicare recommends we use tests and measures published in research: KELS, Dynamometer, Functional Reach Test, MMT, RPE (rating of perceived exertion), goniometric ROM, TUG, BERG, ACL, CPT
Documentation: Focus is YOU • Explain results of tests: i.e. MMT below 3/5, patient is unable to utilize UE for feeding successfully without assistance or would be unable to assist with bathroom transfers
Documentation: Focus is YOU • If no standardized tests used, Medicare recommends functional progress towards goals which is the standard independence scale that we use most often.
Documentation: Focus is YOU • Last option if not using standardized tests per Medicare: “Ask the client- at the present time, would you say that your health is excellent, very good, fair or poor?” Document the response at eval and discharge.
Documentation: Focus is YOU • ICD-9 Choose a code that is close as possible to a 5 digit number = highest level of specificity Main function of codes is to set up screens or filters for medical review, a diagnosis may be used as an item in a medical review They are updated October 1st each year Rehab diagnosis is the impairment based diagnosis relevant to the problem to be treated.
Documentation: Focus is YOU • ICD-9 • Try to use exception codes and complicating Co morbidities (CC) codes, they will qualify a client for caps and exceptions • Be sure to include all of the applicable codes • Some instances the medical diagnosis has an inherent correlation to rehab services i.e. MS • Some diagnosis is associated with the medical diagnosis i.e. CVA
Documentation: Focus is YOU • ICD-9 • V codes are allowed such as V43.64 THR V43.65 TKR V49.75 BKA V 49.66 AEA
Documentation: Focus is YOU • POC (Plan of Care) Document necessity of therapy with: client self reporting, goals, treatment intensity/frequency/duration, certified POC with physician signature in 30 treatment days, identifies procedures and modalities used, outcomes/goals must be measurable/realistic/time limited, potential to return to premorbid status, include discharge criteria and follow up care
Documentation: Focus is YOU • POC (Plan of Care) continued Document intervention requires complex skill level by a clinician Outcome measures and intervention need to change if there is limited change in function Changing of LTG and dates need to have justification documented
Documentation: Focus is YOU • Goals Criteria for being measurable: 1 Performance- client focused, objective, observable behavior (Who/What) 2 Criteria- degree to measure outcome (quality of action) 3 Conditions- when, where, with whom and under what circumstances 4 Time Frame- date, when
Documentation: Focus is YOU • POC (Plan of Care) continued Outcome measures need to have a baseline of function to measure change Standardized test scores alone are not functional performance related to occupation Outcomes need to be measurable and client centered (not written like: therapist will do….)
Documentation: Focus is YOU • Terminology to Avoid Slow progress, little progress noted, patient agitated or confused, unable to learn, disoriented to time and place, poor attention span, no problems noted, little hope for progress
Documentation: Focus is YOU • Suggested terminology Redirected patient behavior, individualized training program to maximize performance, customized treatment approach to match condition of patient, techniques to teach new skill added to program, condition continues to require skilled services, deficits continue to compromise safety, positive results with safety issues addressed
Documentation: Focus is YOU • Treatment Encounter Notes Identify the daily skilled treatment activities and daily modalities provided, identify the professional daily providing the service, use CPT codes that match the treatment provided- timed and untimed codes, the note is the justification for the billing doe on the claim, Medicare assumes the client tolerated the treatment unless there is documentation stating otherwise, client’s response to intervention is a good idea